Download
1 / 1
10 likes | 136 Views
XXXIII Congreso SEMI-11th Congress EFIM RV - 117 THE REFRACTARY HYPERTENSION. PERSPECTIVE FROM A VASCULAR RISK UNIT T. Sanchez-Monton(1), D. Pujol Dominguez(1), J. Vega-Cervantes(1), N. Campillo Guerrero(1), G. Tornel Sanchez(1), M. Jiménez Pascual(1), A. Rodriguez Pavía(1), J. Rodenas Checa(2)

E N D
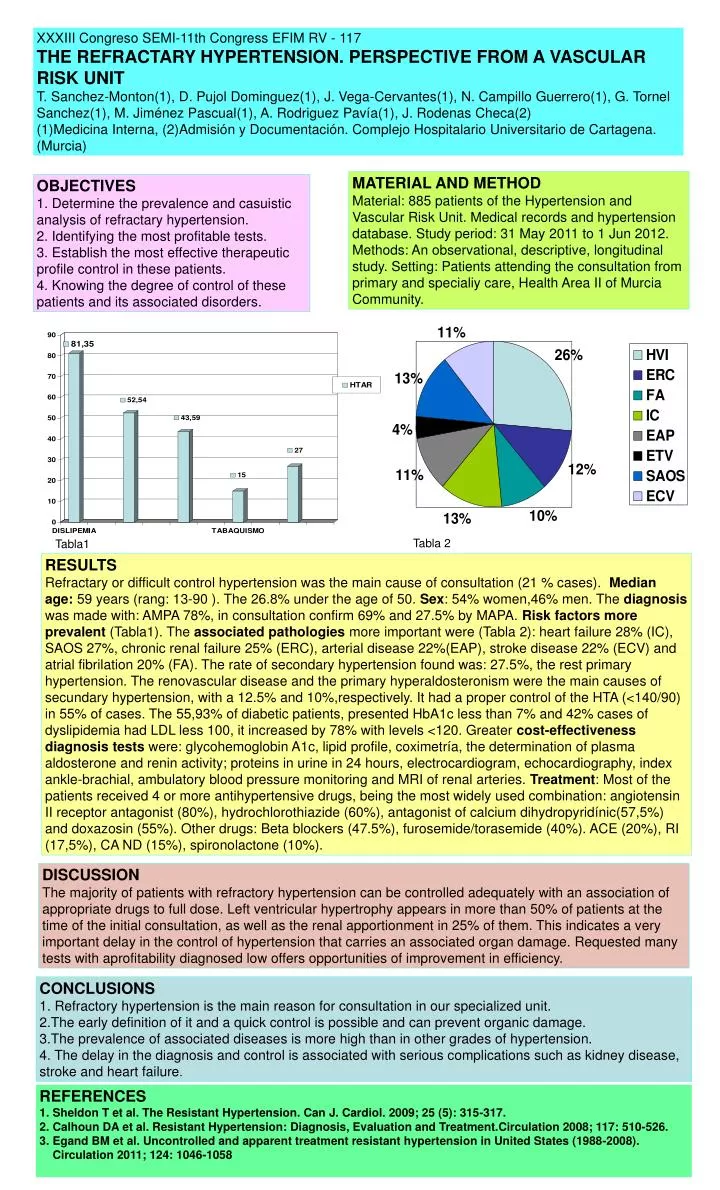
XXXIII Congreso SEMI-11th Congress EFIM RV - 117 THE REFRACTARY HYPERTENSION. PERSPECTIVE FROM A VASCULAR RISK UNIT T. Sanchez-Monton(1), D. Pujol Dominguez(1), J. Vega-Cervantes(1), N. Campillo Guerrero(1), G. Tornel Sanchez(1), M. Jiménez Pascual(1), A. Rodriguez Pavía(1), J. Rodenas Checa(2) (1)Medicina Interna, (2)Admisión y Documentación. Complejo Hospitalario Universitario de Cartagena. (Murcia) MATERIAL AND METHOD Material: 885 patients of the Hypertension and Vascular Risk Unit. Medical records and hypertension database. Study period: 31 May 2011 to 1 Jun 2012. Methods: An observational, descriptive, longitudinal study. Setting: Patients attending the consultation from primary and specialiy care, Health Area II of Murcia Community. OBJECTIVES 1. Determine the prevalence and casuistic analysis of refractary hypertension. 2. Identifying the most profitable tests. 3. Establish the most effective therapeutic profile control in these patients. 4. Knowing the degree of control of these patients and its associated disorders. Tabla 2 Tabla1 RESULTS Refractary or difficult control hypertension was the main cause of consultation (21 % cases). Median age: 59 years (rang: 13-90 ). The 26.8% under the age of 50. Sex: 54% women,46% men. The diagnosis was made with: AMPA 78%, in consultation confirm 69% and 27.5% by MAPA. Risk factors more prevalent (Tabla1). The associated pathologies more important were (Tabla 2): heart failure 28% (IC), SAOS 27%, chronic renal failure 25% (ERC), arterial disease 22%(EAP), stroke disease 22% (ECV) and atrial fibrilation 20% (FA). The rate of secondary hypertension found was: 27.5%, the rest primary hypertension. The renovascular disease and the primary hyperaldosteronism were the main causes of secundary hypertension, with a 12.5% and 10%,respectively. It had a proper control of the HTA (<140/90) in 55% of cases. The 55,93% of diabetic patients, presented HbA1c less than 7% and 42% cases of dyslipidemia had LDL less 100, it increased by 78% with levels <120. Greater cost-effectivenessdiagnosis tests were: glycohemoglobin A1c, lipid profile, coximetría, the determination of plasma aldosterone and renin activity; proteins in urine in 24 hours, electrocardiogram, echocardiography, index ankle-brachial, ambulatory blood pressure monitoring and MRI of renal arteries. Treatment: Most of the patients received 4 or more antihypertensive drugs, being the most widely used combination: angiotensin II receptor antagonist (80%), hydrochlorothiazide (60%), antagonist of calcium dihydropyridínic(57,5%) and doxazosin (55%). Other drugs: Beta blockers (47.5%), furosemide/torasemide (40%). ACE (20%), RI (17,5%), CA ND (15%), spironolactone (10%). DISCUSSION The majority of patients with refractory hypertension can be controlled adequately with an association of appropriate drugs to full dose. Left ventricular hypertrophy appears in more than 50% of patients at the time of the initial consultation, as well as the renal apportionment in 25% of them. This indicates a very important delay in the control of hypertension that carries an associated organ damage. Requested many tests with aprofitability diagnosed low offers opportunities of improvement in efficiency. CONCLUSIONS 1. Refractory hypertension is the main reason for consultation in our specialized unit. 2.The early definition of it and a quick control is possible and can prevent organic damage. 3.The prevalence of associated diseases is more high than in other grades of hypertension. 4. The delay in the diagnosis and control is associated with serious complications such as kidney disease, stroke and heart failure. • REFERENCES • Sheldon T et al. The Resistant Hypertension. Can J. Cardiol. 2009; 25 (5): 315-317. • Calhoun DA et al. Resistant Hypertension: Diagnosis, Evaluation and Treatment.Circulation 2008; 117: 510-526. • Egand BM et al. Uncontrolled and apparent treatment resistant hypertension in United States (1988-2008). Circulation 2011; 124: 1046-1058