Download
1 / 40
500 likes | 1.62k Views
Class Lobosea & Amebic Infections. Entamoeba histolytica E. coli E. gingivalis. Class Lobosea. Intestinal Amebae. Entamoeba E. histolytica (pathogen) E. coli E. gingivalis. Entamoeba Morphology. Ingested RBC. Nucleus with central karyosome and finely divided peripheral chromatin.

E N D
Class Lobosea & Amebic Infections Entamoeba histolytica E. coli E. gingivalis
Intestinal Amebae • Entamoeba • E. histolytica(pathogen) • E. coli • E. gingivalis
Entamoeba Morphology Ingested RBC Nucleus with central karyosome and finely divided peripheral chromatin Pseudopod E. histolytica trophozoite
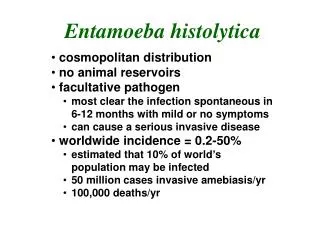
Entamoeba Morphology 1-4 ring-like nucleiwith finely divided peripheral chromatin Cyst wall and round shape Mature E. histolytica Cyst
Entamoeba histolytica Cysts Trophozoites Thick wall Plasmalemma (thin) 1-4 ring-like nuclei 1 ring-like nucleus Chromatoidals Lacking (blunt) Round, 14-20 µm Irregular, 12-17 µm Concentratable Labile Morphologic Comparison
Life Cicle of E. histolytica Amebiasis Transmission • Humans acquire E. histolytica by: • Ingestingcysts in fecally contaminated food or drink • Rarely by directly inoculatingtrophozoites into colon or other sites (anal sex?) • Fecal-Oral transmission (hand to mouth) • Infective cysts and trophozoites pass in feces
E. histolytica Stages - CYSTS • UsualInfective Stage for humans • Resistant walls maintain viability • If moist can last several weeks • Killed by desiccation or boiling • UsualDiagnostic Stage in formed stools • Can be concentrated and stained easily • Not seen in liquid (diarrheic) stools or tissues
E. histolytica Stages - TROPHOZOITES Are the motile, feeding stages that: • Cause amebiasis (damage tissue) • Spread throughout the body, but ... • rarely transmit the infection to others • are labile in liquid stools or tissue, and • must be rapidly found or preserved (quick fixation & cold storage) for laboratory diagnosis
Pathogenesis of Amebiasis Trophozoites ... • Attach to mucosal epithelial cells (MEC) • Lyse MEC • Ulcerate and invade mucosa • Cause dysentery (diarrhea + blood) • Metastasize via blood &/or lymph • Form abscesses in extraintestinal sites
Clinical Classification of Amebiasis (World Health Organization) Asymptomatic (intestinal) Amebiasis "Cyst Passers” • Most common • Infection may continue without clinical symptoms for weeks to months ... • May spontaneously resolve (self cure)/or carrier state Symptomatic Infection: Intestinal Amebiasis: (colon and rectum) Acute Dysenteric (dysentery) Chronic Non-Dysenteric (“self-cured”) Extra-Intestinal Amebiasis: Amebic Liver Abscess (ALA) Amebic Pulmonary Abscess Other sites (brain, skin, GU, ?)
Acute Dysenteric Amebiasis: Amebic Dysentery Symptoms: • Bloody mucoid diarrhea • RBCs and few WBCs (pus) in stools • Abdominal pain • weight loss • bloating, tenesmus and cramps Signs: • Fever (33%) • Diffuse abdominaltenderness • Tender (enlarged) liver • Stools positive for trophozoites +/- WBC • NOT cysts in loose stools
Pathology • Intestinal ulcers are due to enzymatic degradation of tissue. • The infection may result in appendicitis, perforation, stricture granuloma, pseudo-polyps, liver abscess • Sometimes brain, lung and spleen abscesses can also occur. Strictures and pseudo-polyps result from the host inflammatory response.
Amebic abscess of liver • Gross pathology of liver containing amebic abscess • Gross pathology of amebic abscess of liver.
Chronic Non-Dysenteric Amebiasis: “self-cured” carrier state • 37% symptomatic >5 years • Intermittent diarrhea, mucus, abdominal pain, flatulence and/or weight loss • E. histolyticatrophs (rarely cysts) in stools • Positive serology
Intestinal Amebiasis Complications • Intestinal perforation and Peritonitis (a surgical emergency) • Ameboma • Palpable mass of granulation tissue that may obstruct colon • Toxic megacolon • complication of inappropriate steroid therapy
injuries of lungs perforation of diaphragm abscess in liver injury of ascending colon injury of descendingcolon Entamoebasis
Extra-Intestinal Amebiasis: • Amebic Liver Abscess (ALA) • Symptoms • dysentery (1 yr), weight loss, abdominal pain, chest or shoulder pain • Complications • Pulmonary Abscess: by direct extension through the diaphragm into thorax • Rupture into the pleural cavity and/or hepatobronchial fistulas => trophozoites in sputum! • Extension to other sites, including • peritoneum, pericaridum, others • Amebic Pulmonary Abscess • Other sites: brain, skin, urogenital system
DX: Laboratory Diagnosis of Hepatic Amebiasis • Examine stoolsfor trophs/cysts (suggestive) • Blood cell counts - leukocytosis? • Radiologic Studies • Serologic tests • Catheterize abscess and aspirate: Examine "anchovy paste" aspirate for trophozoites and do serologic testing for amebic antigens • Culturefor other pathogens (sterile on first stick, then contaminants) • Chemotherapeutic Trial
Diagnosis of Intestinal Amebiasis Techniques: • Direct Fecal Smear (trophs and cysts) • Fecal concentration techniques - (cysts) • Permanent Stained Fecal Smear • Serologic Tests (for chronic disease)
E. histolytica: Microscopy • Entamoeba histolytica trophozoites in section of intestine • Entamoeba histolytica cyst and trophozoite, haematoxylin stained 1 2
Prevention/Control of Amebiasis Individual measures • Diagnosis and treatment of E. histolytica patients • no animal reservoirs (other than humans) are known • Safe drinking water (boiling or 0.22 µm filtration) • Cleaning of uncooked fruits and vegetables • Prevention of contamination of food
Prevention/Control of Amebiasis Community measures • Public services and utilities • Adequate disposal of human stools • Safe and adequate water supply • Primary health care systems • Health education (washing hands, cleaning and protecting food, controlling insects) • Specific surveillance programs and Control programs integrated into ongoing sanitation & diarrhea control • Health Regulations • Control of food vendors and food handlers • Control of flies and cockroaches
food vacuole nucleus Entamoeba coli • It is a commensal of the human large intestine, but it looks much like E. histolytica • Cyst usually has 8 nuclei • Does not produce the protein-degrading [proteolytic] enzymes
Red blood cells amoeba Entamoeba gingivalis
Entamoeba gingivalis • lives in/on the teeth, gums, and sometimes tonsils. • it measures 10-35 µm in length • is present in all cases of active periodontitis • does not produce the cysts
Infections with Free Living Amebae Naegleria fowleri Acanthamoeba spp.
Free Living Amebae Not seenin humans Naegleria Acanthamoeba cysts & trophs are seen in humans
Life cycle of Naegleria fowleri • 1 – cyst, • 2 – amoeba makes it way into cranium, • 3 – switches to flagellate in order to swim into mouth or nose.
Primary Amebic Meningoencephalitis PAM An acute suppurative infection of the brain and meninges that is rapidly fatal and usually not diagnosed antemortum • Caused by Naegleria spp. • Headache, lethargy and olfactory problems • Sore throat, runny nose, severe headache, vomiting, stiff neck, confusion leading to ... • Coma and death
Primary Amebic Meningoencephalitis PAM Thermophilic, chlorine tolerant trophozoites penetrate cribiform plate and follow olfactory nerves into brain ... • Acute inflammation and hemorrhagicnecrosis • Sanguinopurulent exudate containing trophs is found in meninges & tissues • CSF: Glucose -, Protein +, Leukocytes + • NEG Gram stains and bacterial CSF cultures
Acanthamoeba spp. Acanthamoeba trophozoites with acanthopodia
Acanthamoeba • are found in the soil and dust, in fresh water (lakes, rivers, and hot springs and in hot tubs. • may also be found in sea water • can also be found in contact lens paraphernalia • Acanthamoeba have been found in the nose and throat of healthy people as well as those with compromised immune systems.
Acanthamoeba • can enter the skin through a cut, wound, or through the nostrils • can travel to the lungs and through the bloodstream to other parts of the body, especially the central nervous system. • can enter the eye via contact lenses or through a corneal cut or sore. Infection, keratitis or a corneal ulcer results. • In addition, it can cause skin lesions and/or a systemic (whole body) infection!!!
Acanthamoeba Keratitis Corneal infection with Acanthamoeba spp. trophozoites & cysts • Ulcerations & “Ring Infiltrate” of cornea • Induced by • trauma to eye, exposure to contaminated H2O • contact lens wear with tap water rinsing • Cavorting in hot tub wearing soft-contacts!
Granulomatous amebic encephalitis (GAE) • Acanthamoeba spp. cause a serious, most often deadly infection called GAE • Symptoms: headaches, stiff neck, nausea and vomiting, tiredness, lack of attention to people and surroundings, loss of balance and bodily control, seizures, and hallucinations. • Signs and symptoms progresses over several weeks and death usually occurs.