Download
1 / 19
200 likes | 252 Views
This discussion covers alveolar proteinosis, detailing its clinical symptoms, diagnostic methods, treatment options including whole-lung lavage, and prognosis. Learn about this rare respiratory condition and its impact on lung function.

E N D
Introduction • Intra-alveolar accumulation of lipid and proteinaceous material. • Secondary to impaired clearance of surfactant by alveolar macrophage. • Increased work of breathing • Diminished surface area for gas diffusion • Ultimately respiratory failure. • Not associated with inflammation and lung architecture is typically preserved.
Introduction • Frequency: 3.76 cases per million • Race: no race predilection • Sex: male/female: 2.65/1, 72% with smoking • Non-smoker: no male predominance • Age: peak:30~50y/o, median age at diagnosis: 39y/o
Etiology • Congenital PAP • Autosomal ressive pattern • Mutation in the genes for (1) surfactant protein B or C, (2)beta chain of receptor for GM-CSF • Secondary PAP: unknown etiology • In association with lysinuric protein intolerance • Inciting agents: aluminum, titanium, silicates, insecticides • Acquired PAP: unknown etiology • GM-CSF neutralizing autoantibody in serum and BAL fluid
Clinical symptoms • Neonatal respiratory distress • Progressive respiratory failure and marked hypoxemia shortly after birth • Prolonged ventilator dependence: slow resolution, persisting atelectasis, pneumonia • Dyspnea: • Most consistent finding in children and young adults • 50~80% • Cough: • Occasionally with thick sputum or solid material • 80%
Clinical symptoms • Failure to thrive: • More common in young children and infants • Decreased level of activity and difficult feeding • Uncommon symptoms: chest pain, fever, pneumothorax, hemoptysis
Lab studies • Arterial blood gas analysis • Low PaO2 • Compensated respiratory alkalosis • Latex agglutination test: 100% sensitivity, 98% specificity • Pulmonary function test • Mild restrictive pattern of lung disease • Slightly diminished functional lung volumes • Decreased DLCO
Bronchoalveolar lavage • Milky or opalescent aspirate with large alveolar macrophage and increased lymphocytes • Positive for PAS • Elevated SP-A and SP-D • Low level of SP-B
Lung biopsy • The criterion standard for diagnosis • Transbronchial biopsy: not enough tissue for diagnosis in children • Pathologic finding: • Granular, proteinaceous, fluid-filled alveolar spaces • Cholesterol crystals are sometimes observed • Alveolar structure is generally preserved • Some thickening of interlobular septae • EM: • lamellar bodies and tubular myelin within the alveolar space • Adds little to the diagnosis
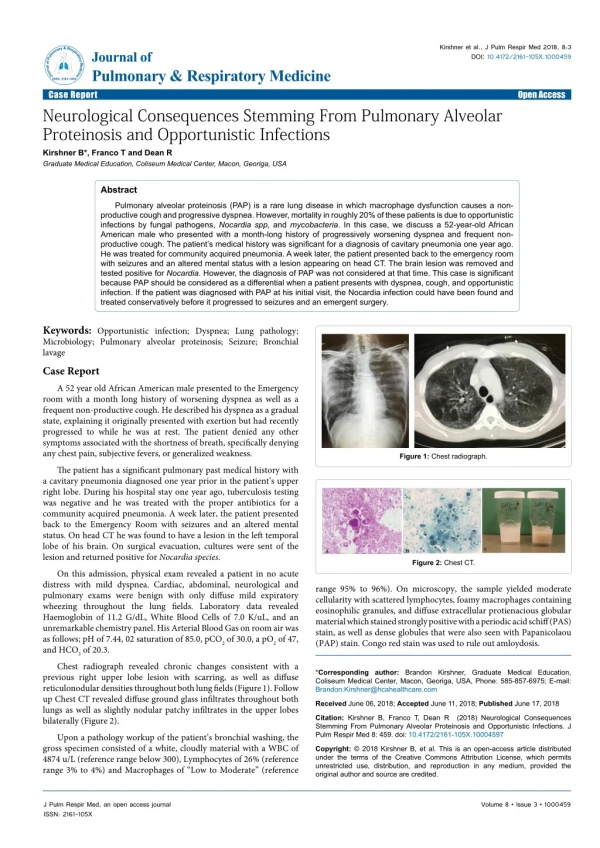
Image--CXR • Bilateral symmetric air-space opacity, ground-glass appearance • perihilar or basilar predominance("bat wing" distribution) • Air bronchograms are uncommon. • No mediastinum widening, adenopathy, cardiomegaly, pleural effusions.
Image--CT scan • Conventional CT: bilateral areas of consolidation and reticulation • HRCT • Crazy paving: patchy, bilateral, geographic areas of ground-glass opacity associated with interlobular septal thickening • Interlobular septal thickening : more frequent in the lower lung zones
Differential diagnosis • Hemosiderosis • Hypersensitivity pneumonitis • Goodpasture syndrome • Pulmonary alveolar microlithiasis • Sarcoidosis • Lymphoma • Bronchioalveolar cell carcinoma
Treatment • Mechanical ventilation • necessary in children with congenital PAP • Partial liquid ventilation (PLV) offers the advantage of lung lavage combined with ventilator support. • Gene therapy • Intravenous immunoglobulin (IVIG) and GM-CSF therapy
Treatment • The mainstay of therapy in PAP is whole-lung lavage • improved survival rates • < 20 y/o: 58% response>40 y/o: 90% response • Remove surfactant buildup or minimize the effect of macrophage dysfunction • Other options: extracorporeal membrane oxygenation and lung transplantation
Mortality/Morbidity • Neonate with congenital alveolar proteinosis • With conventional therapy:100% • Lung transplantation: 5-year survival rate:88±4% • Pulmonary alveolar proteinosis: • <5 y/o: 14±13% • Children with late-onset disease: bets likelihood for survival
Prognosis • Highly variable course with clinical and radiological episodes of exacerbation and remission • 50% improvement/recovery • 30% death