Download
1 / 6
60 likes | 220 Views
This overview presents findings from the ENESTnd study, comparing the efficacy and safety of Nilotinib (300 mg and 400 mg BID) with Imatinib (400 mg QD) in chronic myeloid leukemia treatment. Notable endpoints include the primary measure of major molecular response (MMR) at 12 months, showing superiority of Nilotinib. Data on long-term follow-up highlights cardiovascular events, emphasizing the incidence of IHD and PAOD. Key genetic factors such as CYP3A4/5 metabolism are also examined, implicating their role in treatment outcomes and patient stratification.

E N D
SPIRIT3 support includesBiobanking: broadly as for SPIRIT2, but plus genomic DNA (mouth wash via kit)Correlative Science: BiomarkersLSC biologyNGS: mutation analysis: hypothesis generation
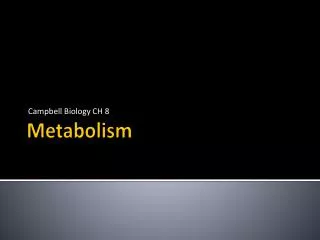
Example: Imatinib Metabolism St John’s Wort carbamazepine phenytoin CYP3A4/5 ketoconazole erythromycin grapefruit juice CGP-74588 (t½ = 40hrs) imatinib (t½ = 18hrs) CYPs: 1A1, 1B1, 1A2, 2D6, 2C9, 2C19 NQO1 &2 TXN minor metabolites GSTs NATs, UGTs cell damage EXCRETION EXCRETION ROS DNA damage
GSTT1{del} and GSTM1{del} Results n = 77 Mantel-Cox Log Rank Test (p values) n = 88 n = 17 n = 11 p < 0.000 Davies et al 2012, EHA Amsterdam (abstract)
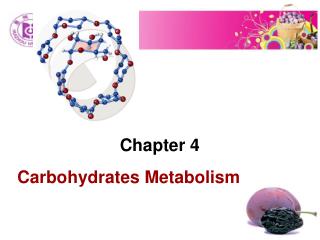
ENESTnd: Study Design R A N DO M I S ED * Nilotinib 300 mg BID (n = 282) • N = 846 • 217 centres • 35 countries Nilotinib 400 mg BID (n = 281) Imatinib 400 mg QD (n = 283) * Stratification by Sokal risk score. 10 years of follow-up are planned Primary endpoint = MMR at 12 months. This is superior in nilotinib recipients (either dose) compared with imatinib (P < .0001; Saglio et al NEJM 2010). Kantarjian HM, et al. Blood. 2012;120(21):[abstract 1676].
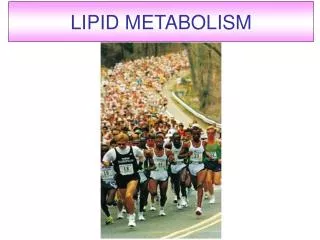
Arterial Events by 3 Years (All Grades) • IHD, ischaemic heart disease; PAOD, peripheral arterial occlusive disease. • 11/23 IHD events occurred between years 2 and 3 (4 on nilotinib 300 mg BID, 5 on nilotinib 400 mg BID, 2 on imatinib) • 3 patients on nilotinib 400 mg BID discontinued study drug due to IHD • 2/7 PAOD events occurred between years 2 and 3; both occurred on nilotinib 400 mg BID • 6/7 patients (85%) with PAOD had pre-existing risk factors at baseline • No patient discontinued because of PAOD • No patient at any time on study in either nilotinib arm had a QTcF > 500 ms or LVEF < 45% LVEF, left ventricular ejection fraction. Data cutoff: 27Jul2011.
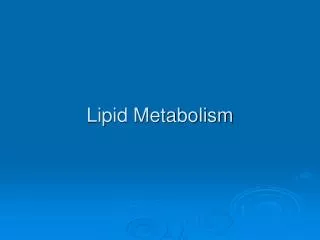
ENESTnd: arterial Events by 4 Years Including cerebrovascular events: 18 24 4 • Between years 3 and 4, five new patients had an IHD event (2 in the nilotinib 300 mg BID arm and 3 in the nilotinib 400 mg BID arm), and 2 new patients had a PAOD event (both in the nilotinib 400 mg BID arm) • 1 patient in the nilotinib 400 mg BID arm with previously reported PAOD had a newly reported drug-related SAE (arterial stenosis limb) leading to treatment discontinuation Data cutoff: 27Jul 2012.