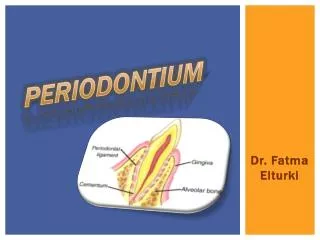
PERIODONTIUM
PERIODONTIUM. Dr. Fatma Elturki. Objectives. The gingiva:- Macroscopic Appearance of the Gingiva. Histology of Gingiva. The Dentogingival Junction. Development of junctional epithelium. Shift of the Dentogingival Junction. Bone tissue and alveolar process:-

PERIODONTIUM
E N D
Presentation Transcript
PERIODONTIUM Dr. Fatma Elturki
Objectives The gingiva:- • Macroscopic Appearance of the Gingiva. • Histology of Gingiva. • The Dentogingival Junction. • Development of junctional epithelium. • Shift of the Dentogingival Junction. Bone tissue and alveolar process:- • Structural constituents. • Types of bone. • Incremental lines of lamellated bone. • Alveolar process and its structure. • Age changes.
Gingiva • The gingiva is a pink strip of oral mucosa which surrounds the cervical zone of the teeth and is attached to it and to the coronal part of alveolar bone. • It extends from the dentogingival junction to the mucogingival junction. • The gingival is not only part of the oral mucosa but also compost the marginal periodontium.
Macroscopic Appearance of the Gingiva • Morphologically the gingiva can be divided into: (a) the free or marginal gingiva. (b) the attached gingiva and. (c) the interdental papillae.
The free gingiva • It is not actually free, but is delicately attached to the tooth surface. • It is the first part or the marginal part of the gingiva so; it surrounds the cervical part of each tooth. • It is separated from the teeth by a fine space called the gingival sulcus. And so, the free gingiva has an oral surfaceand a dental surface. • The oral surface faces the facial and the oral cavities. It begins from the gingival margin and ends at the free gingival groove. The free gingival groove demarcates the free from the attached gingiva. • The dental surface lined by the gingival sulcus and faces the toil It begins from the gingival margin and ends at the junctional epithelial
Gingival sulcus • The gingival sulcus is a shallow space extends from the gingivalmargin into the junctional epithelium. • Its depth is from 0.5-2 mm. • Its epithelium (the dental surface) may act as semipermeable membrane though which the gingival fluid pass into the sulcus and the bacterial antigens pass into the gingiva. • The gingival sulcus contains gingival fluid, plaque and calculus.
The Attached Gingiva • It is firmly attached to the cervical parts of the tooth and to the underlying alveolar bone by the gingival fibers and the junctional epithelium. • The attached gingival mucosa lies between the free gingiva and the alveolar mucosa. It is separated from the former by the free gingival groove and from the latter by the mucogingival junction. • The width of theattached gingiva is not uniform through the oral cavity. It is widest in the region of the upper anterior teeth (5-6mm.) and narrowest in regions of the lower molar teeth (3mm.). There is no attached gingiva at the palatal gingiva.
The Attached Gingiva • In a healthy mouth, the attached gingiva shows signs of stippling (orange-peel appearance) which is not found in other areas of the oral mucosa. • The degree of stippling and the texture of the collagenous fibers vary according to age and sex. • The absence of stippling, which is brought about by edema of the tissue, can be considered as initial sign of pathology
The Interdental Papilla • It is that part of the gingiva that fills the space between two adjacent teeth. In cases where there is no contact area, the interdental papilla is reduced. It is formed of the free and attached gingivae. • The free gingivae facially and orally are attached to each other by the interdental col. The interdental col is a valley like depression of the mucous membrane connecting the two free gingivae (facially and lingually) below the contact area.
The Interdental Papilla • When viewed from the lingual and facial aspects, the interdental papilla forms a triangular tissue and called gingival papilla. Sometimes the labial surface of the attached gingiva labially shows melanin pigment especially in dark skinned races. • When viewed from the lingual and proximal aspects, the interdental papilla is pyramidal between the anterior teeth while it is tent shaped in the posterior region. • With age, the vestibular and oral interdental edges, descend and the area of the col is flattened.
Histology of Gingiva • The gingiva is formed of surface epithelium and underlying lamina propria The surface epithelium :There are three types of gingival epithelium according to the behavior of keratin. Orthokeratinized epithelium: stratum corneum consists of flat tightly packed horny scales and the nuclei are completely absent. This type constitutes 15%. Parakeratinized epithelium: the stratum corneum consists of flat horny scales, which retain pyknotic nuclei or remnants of nuclear material. This type constitutes 75%. Nonkeratinized epithelium: the stratum corneum is absent. This type accounts for about 10%. Such gingiva is considered normal, the sheltered areas of the gingiva are always nonkeratinized, these are the epithelial lining of the gingival sulcus and the epithelium of the col.
Histology of Gingiva • The lamina propria: it is made up of dense connective tissue composed of bundles of collagenous fibers, fibroblasts, blood vessels, lymphatics and nerves. • The lamina propria consists of papillary layer and a reticular layer. • The papillary layer is formed of tall, numerous and slender papillae. Few elastic fibers are confined to the walls of blood vessels. The texture of these fibers is fine in the young and tends to increase in coarseness with the advance of age. • The reticular layer is formed of the same kind of tissue, the fibers being arranged in a delicate network. • In the attached gingiva, the fiber bundles, which arise from the cementum and alveolar crest radiate to the papillary layer of the gingiva further, strengthen the attachment of the .gingiva. Lamina propria
Interdental ligament Cross-sectioned tooth Interdental papilla — Cementum lamina propria • The gingival ligament is functionally oriented in the following groups: • Dentogingival group. • Alveologingival group. • Circular group. • Dentoperiosteal group. • Transseptal fiber system.
lamina propria • The cellular elements of the lamina propria are mainly fibroblasts. These are found in the free gingiva where the fibers are more finely textured. • Presence of plasma cells and lymphocytes are not uncommon in theclinically normal gingiva, especially near the bottom of the gingival sulcus. These cells have an important function in the defense mechanism of the body and in repair. • Mast cells are found in the gingival connective tissue in a great number, however, the function of mast cells in the gingiva remains speculative. • It has to be noted that in the gingiva a definite layer of submucosa cannot be recognized, instead the dense fibers of the lamina propria fuse with the periosteum of the alveolar process or cementum at the cervical region.
Blood and nerve supply • The main blood supply is derived from the interdental arteries which penetrate the interdental septa, perforate the alveolar crest and end in the gingiva of the interdental papilla as well as in the adjacent areas of the buccal and lingual gingiva. • In addition superficial branches of the lingual, buccinator, mental and palatine arteries supply also the gingiva. • Blood vessels are accompanied with lymph vessels, which drain in the submental and submandibular lymph nodes. • The human gingiva is well innervated.
The Dentogingival Junction • This is the junction of the soft gingival tissue, (epithelium andlamina propria) and the hard dental tissue (enamel and cementum). • The sealing of this junction is the function of the junctional epithelium or attachment epithelium. The epithelial component of the dentogingival junction is divided into three functional components which arethe gingiva including the gingiva margin (firmness & protective), & gingival sulcus (protective) and the junctional epithelium (sealing). • The connective tissue component is divided into superficial and deep tissues.
The junctional epithelium (Attachment epithelium) • Junctional epithelium is the apical extension of the sulcular epithelium. • It begins at the bottom of the gingival sulcus and extends apically along the tooth surface where it stops at any point on the tooth surface to seal it. • N.B: The length of the attachment epithelium may extend up to 2mm.
Histologically • The junctional epithelium is composed of nonkeratinized stratified squamous epithelium without ridges or pegs. • The apical end of the junctional epithelium is formed of 3 to 4 cell layers, while its coronal end is thicker, formed of 15 to 30 cell layers. • The junctional epithelium is consisted of two zones: a basal celllayer of cuboidal cells and several layers of flatten cells. The suprabasalcells are aligned parallel to the tooth surface and they cells are mitotically inactive. The intercellular spaces are wide and are occupied byneutrophils, leucocytes, and mononuclear cells. • The interface between it and the connective tissue is smooth without epithelial ridges
II- Connective Tissue Component Of the dentogingival junction • The connective tissue supporting the junctional epithelium is structurally different from connective tissue supporting the oral gingival epithelium in that, even in clinically normal gingiva, it contains a population of inflammatory cells which migrate into both the junctional and the sulcular epithelium to appear between the gingival sulcus cells and eventually in the gingival fluid. • .The gingival and the sulcular components are supported by superficial connective tissue (instructive for normal maturation). While, the junctional epithelium is supported by deep connective tissue (instructive for nourishment). superfacial CT Deep CT
Gingival sulcus •Enamel Cell turnover in junctional epithelium Junctional epithelium turnover • The junctional epithelium has a high rate of cell turnover, approximately 4-6 days. Since its surface cells are specialized for the attachment to the tooth. So, it is difficult to be eliminated through it. So, it has to migrate from the basal cells apically and then migrate in a coronal direction paralleling the tooth surface to be sloughed off into the gingival sulcus.
Development of junctional epithelium • As eruptive movement begins, the enamel of the crown is covered by reduced enamel epithelium (REE). • As the tooth moves through the eruption pathway , the REE cells secrete proteolytic enzymes that degrade the connective tissue separating it from the oral epithelium. • As the tooth approaches the oral mucosa the REE and oral epithelium proliferate and fuse, forming a layer of epithelial cells over the crown tip . Clinically, the mucosa becomes blanched because of a lack of blood supply to the area.
Development of junctional epithelium • The central cells in this epithelial layer degenerate, creating an epithelial-lined canal through which the crown will emerge into the oral cavity without exposing the surrounding connective tissue and without bleeding. • When the tooth erupts through the oral mucosa, its REE becomes the initial Junctional epithelium of the dentogingival junction.
Shift of the Dentogingival Junction • Gradual exposure of the clinical crown is accomplished through axial movement of the tooth (active eruption) and through separation of the junctional epithelium from the crown (passive eruption). • The part of the tooth seen in the oral cavity and bathed in saliva or part of the tooth coronal to the attachment epithelium is termed (clinical crown). • It may be shorter, equal or larger than the (anatomical crown) which is the part of the tooth covered by enamel
Shift of the Dentogingival Junction • The crown exposure involving passive eruption and further recession has been described in four stages: First Stage: Here we find coronal end of the attachment epithelium is on the enamel, while the apical end of the attachment epithelium remains on the CEJ. In this stage the clinical crown is shorter than the anatomical crown. This stage persists in the primary teeth. In permanent teeth it is found nearly till the age of 20 or 30 years.
Shift of the Dentogingival Junction II. Second Stage: In this stage the coronal end of the attachment epithelium is still on the enamel while the apical end had shifted to the cervical part of the root cementum. Here too the clinical crown is short than the anatomical crown. This stage is generally seen between 25-40 years or even later. III.Third Stage: In this stage the coronal end of the attachment epithelium is at the CEJ. The apical end is on the root cementum. This stage is transitory because the epithelium shifts gradually along the tooth surface and the attachment epithelium does not the linear cemento-enamel junction for a long time. The clinical crown is equal to the anatomical crown.This stage is generally seen above 40 years
Shift of the Dentogingival Junction IV. Fourth Stage: The entire attachment epithelium is present on root surface i.e., both the coronal and apical ends are attached to the cementum of the root. In this stage part of the cementum of the root isuncovered and exposed to the oral cavity. The clinical crown is longer than the anatomical crown.
Bone tissue & Alveolar process
BONE TISSUE • Bone is a specialized type of connective tissue with calcified intercellular substance. • Bone has a complex structure and function. The structure of bone is adapted to mechanical stresses.
Structural constituents The structural constituents of bone tissues are • Cells. • Matrix (fibers and ground substance). • Mineral salts.
Bone cells • In developing as well as mature bone, four species of bone cells are recognized, • osteoprogenitor cell. • osteoblasts. • osteocytes, and • osteoclasts.
Bone Matrix (Organic constituents) • Bone matrix consists of different organic materials that form about 35% of the bone composition. • The major constituent is the collagen fibers which lie in a ground substance of glycoproteins and proteoglycans with small amount of growth factors and lipids.
Minerals (Inorganic material) • The inorganic material almost consists of calcium and phosphate in the form of hydroxyapatite crystals that forms about 65% of the bone composition.
Types of bone Bone tissue mainly exists in three forms: • Lamellar bone: • Compact bone. • cancellous or Spongy bone. • Non lamellar bone • Coarse fibered bone (Woven bone). • Bundle bone.
Lamellar bone • This type of bone is subdivided into two types, compact bone and cancellous bone.
compact bone • These lamellae disposed around a central channel containing blood vessels, lymphatics and nerves. • This channel isknown Haversian canal and with its concentric lamellae form: Haversian system (osteon). • As a result of the continuous resorption and redeposition of bone, complete newly formed Haversian systems are disposed between partly resorbed systems formed earlier. The remnants of old Haversian systems form irregular interstitial lamellae between intact Haversian systems.
compact bone • At the outer aspect of compact bone, concentric lamellae had laid-down at the bone surface by osteoblasts of the periosteum which are known as outer circumferential lamellae. At the inner medullary aspect, similar but irregular inner circumferential lamellae merge with trabeculae of cancellous bone
Cancellous bone • Cancellous bone is built up of many spicules and trabeculae surrounding the marrow spaces. • Each trabecula consists of one or more lamellae with lacunae containing osteocytes between them.
Woven bone • The embryonic bone also called immature or coarse fibrillar bone which is characterized by the greater number, of the osteocytes.. • The reduced volume of calcified substance, render this immature bone more radiolucent than mature bone. • Appearance of bone in X-ray occurs 2-3 weeks after actual formation of lamellar bone
Bundle bone • It differs from woven bone in that it contains thick collagen bundles arranged parallel to each other. • Its rate of formation is slow resulting in resting lines between adjacent lamellae. • Bundle bone is characterized by attachment of ligament or tendon to its surface . • Bundle bone contains less mature, course, fewer intrinsic collagen fibrils in the intercellular substance than the mature lamellated bone. • Bundle bone present at inner wall of alveolar socket.
The Periosteum • All the bones of the body are covered externally by a tough membrane of specialized dense connective tissue called periosteum. • The periosteum is attached to the bone by coarse connective tissue fibers called the Sharpey's fibers, while periosteum itself acts as a medium for attachment of the muscles and tendons, as well as, it performs a nutritive function to the underlying bone.
The Endosteum • Is a thin fibrocellular layer of connective tissue, similar in character to the inner layer of the periosteum, it lines the medullary surface of bones.
Incremental lines of lamellated bone • In both compact and spongy bone two types of lines mark the successive layers of bone: Resting lines: • These are slightly straight lines seen in decalcified and ground bone sections. In decalcified sections, stained with H&E., they show dark blue lines. They demonstrate the incremental pattern of bone formation.
Incremental lines of lamellated bone Reversal lines: • These are scalloped lines, which indicate the post osteoclastic activity occurring on the surface of bone undergoing resorption. After osteoclastic activity new bone is laid down by osteoblasts over the old bone. Both old bone and new bone are separated by a scalloped line, which is the reversal line, with the convexity of this line, usually, is directed towards the old bone.
Alveolar bone Development of alveolar bone:- • Near the end of the second month of fetal life the maxilla as well as the mandible forms a groove that is opened towards the surface of the oral cavity. This groove is formed by the growth of the outer and inner plates of the body of the maxilla and mandible. • The tooth germs are contained in this groove together with the alveolar nerves and vessels. Gradually bony septa develop between the adjacent tooth germs. So each tooth is contained in a separate crypt (bony crypt) • Alveolar bone develops from dental follicle. • The ectomesenchymal cells of dental follicle differentiated into osteoblasts and lay down the bone matrix called osteoid.
ALVEOLAR PROCESS • The alveolar process may be defined as that part of the bone of the jaw (mandible or maxilla) that forms and supports the roots of the teeth.
Alveolar process • The development of alveolar bone is dependent on root formation. • Continued presence of alveolar bone appears to require the presence of the tooth; after tooth extraction some alveolar bone is lost, and in edentulous individuals the alveolar bone may be resorbed down to the basal bone.
structure of the alveolar process • Adult alveolar process composed of two parts: • Alveolar bone proper. • Supporting bone.
Alveolar bone proper • Alveolar bone proper is that part of alveolar bone that lines the socket. • It is a thin lamella of compact bone in which periodontal fibers are embedded. • It is specialized type of compact bone composed of bundle bone and Haversian bone • It is referred to as bundle bone because it regularly penetrated by Sharpey's fibers of the PDL.
Alveolar bone proper • It is perforated by numerous minute foramina (Volkman's Canals) that carry branches of the interalveolar nerves and blood vessels into the periodontal ligament and that is why it is called the cribriform plate. • The term lamina dura is given to this layer of bone from its dense radiopaque appearance in X-ray This due to the presence of thick bone without trabeculation that x rays must penetrate and not to any increased mineral content.