Download
1 / 22
230 likes | 429 Views
ASD AND PS. PHYSIOLOGY. ps reduces shunt shunt increases gradient on pulmonary valve. Types of ASD according to Edwards. Secundum type-level of the fossa ovalis Sinus venosus type-associated with anomalous return of right upper pulmonary vein Ostium primum ASD

E N D
PHYSIOLOGY • ps reduces shunt • shunt increases gradient on pulmonary valve
Types of ASD according to Edwards • Secundum type-level of the fossa ovalis • Sinus venosus type-associated with anomalous return of right upper pulmonary vein • Ostium primum ASD • Raghib type-absent coronary sinus with Left SVC connection to left atrium. • Multiple coalescent defects-essentially forming common atrium
Tests • clinical • Ecg p, pr, qrs • cxr
Incidence, Age at Presentation, Clinical • 10 percent CHD, 3:2 male:female • Variable age, according to type. May be asymptomatic into adulthood. • Murmur on preschool physical exam. • Cyanosis in the Raghib type. • Adult with ASD and Rheumatic mitral valve disease=Lutenbacher syndrome. • Auscultation shows wide fixed splitting of the P2 sound with pulmonary flow murmur.
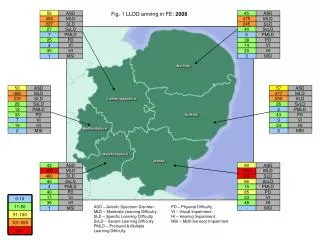
Radiology • Prominent central PA's • Peripheral pruning of vessels with pulmonary hypertension • Prominent RV outflow tract may encroach on the retrosternal space • Left atrium NOT enlarged because the LA can decompress into RA via the defect. • Angiography-presence of mixing at the atrial level is inferred when an indistinct left atrial border is observed on the levophase of a right ventricular injection.
Other tests • CT • rt side heart • pulmonary artery • Contrast spiling into LA • Rt heart cath sats pa pressure • Lt heart cath indications for coronaries
Complications • Eisenmenger • Paradoxical embolism
Patent Foramen Ovale • The defect in patent foramen ovale is not a result of missing tissue; therefore, very specific hemodynamics must be present (ie, right atrial pressure exceeding left atrial pressure) for shunting to occur. • Patent foramen ovale is not associated with an increased risk of endocarditis. Antibiotic prophylaxis is not indicated.
CVA • When patent foramen ovale & unexplained neurologic event Aspirin in low-risk patients or combined with warfarin in high-risk. • The recurrence rate of stroke or transient ischemic attack has been reported to be as high as 3.4-3.9% per year. • In patients with atrial septal aneurysm and patent foramen ovale, the risk of recurrent stroke within 2 years is ~9%,
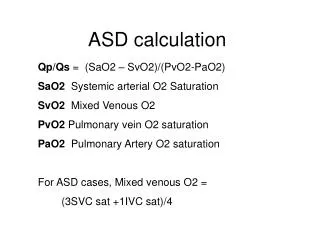
How to calculate shunt • How to do shunt calc • Echo • Pulmonary and Aortic valve areas and flows • (Pva * Pvf) /(Ava * Avf) • Sats • Shunt = (Smix-Sra)(Sart-Smix)
When to close ASD? • Shunt >2:1 • PA pressure • CVA/TIA • AF / arrthymias • Exercise tolerance • Occupation eg diver
RV modelling • In those with severe or long-standing valvular obstruction, infundibular hypertrophy may cause secondary obstruction when the pulmonary valve is successfully dilated. • This frequently regresses over time without treatment. • Some have advocated transient pharmacological b-blockade, but there is insufficient information to determine whether this is effective or necessary.
Doing the op • Pledga, fibb for asd • Beating heart for PV
Q’s • Can do TV on beating heart why not ASD • patch or not to patch ASD • Why small aorta • Why split sounds still present post op
Problems • Low co post op • Tamponade cxr echo clinical • RCA air damage ecg echo • Pulmonary hypertension take patch off