Download
1 / 25
250 likes | 630 Views
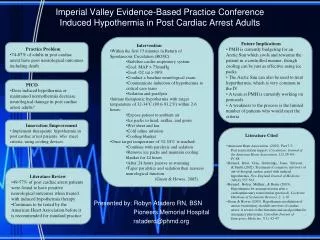
Time and Temperature is Brain: Mild Therapeutic Hypothermia for Post Cardiac Arrest Syndrome. Scott M. Silvers, MD Mayo Clinic Jacksonville Department of Emergency Medicine 2008 American Academy of Emergency Medicine Scientific Assembly FERNE Symposium February 8, 2008. Case.

E N D
Time and Temperature is Brain:Mild Therapeutic Hypothermiafor Post Cardiac Arrest Syndrome Scott M. Silvers, MD Mayo Clinic Jacksonville Department of Emergency Medicine 2008 American Academy of Emergency Medicine Scientific Assembly FERNE Symposium February 8, 2008
Case • November 11, 2007 at 0155 hours • Patient is a 26yo male found unresponsive in a pool of vomit by a friend in a corner of a garage where he was spending the night. • Unknown downtime • EMS was called and found patient 's pupils fixed and dilated upon arrival, and there has been no spontaneous movement. • He was treated with multiple drugs including Narcan, glucose (secondary to a low glucometer reading), epi, atropine, lidocaine, and bicarb. • He was reportedly shocked x 2 for VFib and arrived bradycardic and hypotensive with a faintly palpable femoral pulse.
Case • ET tube placement confirmed by auscultation and ETCO2. Patient's pupils fixed and dilated, no spontaneous movement. No corneal reflex. • Temperature 33 °C. Accu-Check, 200+. • The patient received 1 hour of continuous CPR with defibrillation for VF and multiple doses of ACLS drugs (see CPOE record and nursing notes) • VF ocurred intermittently with asystole • Ultrasound of his heart during this time revealed no spontaneous movement. • Finally, after a bolus of vasopressin and forceful CPR, the patient developed a bradycardic rhythm and weak pulse. • Critical-care transported patient to the unit..
Question • Can we offer anything more to improve the outcome beyond hemodynamic stabilization?
Arctic Sun Cooling System Application of Pads Continuous temperature feedback with bladder thermister
Hospital Discharge • 12/19/07 (5 week stay) • 26-year-old male who was found unresponsive at a friend's house after consuming cocaine and benzodiazepines. • He was dependent on mechanical ventilation for a week as well as vasopressors and dialysis • A tracheostomy was performed. • After 2 days, we were able to discontinue the oxygen support, and the patient was able to breathe with good saturations through the tracheostomy.
Hospital Discharge • He was weaned off vasopressors. • Nephrology concluded that he would be able to be discharged without requiring further dialysis. • The patient was discharged afebrile, hemodynamically stable, with no electrolyte imbalances, with a normal urinary pattern and without any respiratory issues.
Background • “Post Resuscitation” vs “Post Cardiac Arrest” • 1953 First large multi-center report (N = 672) • Adult inhospital cardiac arrest survival = 50% • 2006 National Registry of CPR • N = 19,819 adults; N = 524 children • Adult inhospital cardiac arrest survival = 67% • Children inhospital cardiac arrest survival = 55% • 2007 AHA Statistics • Adult OOH cardiac arrest survival = 6.3% Ann Surg. 1953;137(5):731-744. JAMA. 2006;295(1):50-57. JAMA. 1966;198(4):372-379.
Post-Cardiac Arrest Injuries • Brain Injury • Myocardial dysfunction • Systemic ischemia / reperfusion response • Unresolved pathologic process leading to cardiac arrest
Post-Cardiac Arrest Barriers to Care • Pre-hospital and Hospital providers • Multiple hospital disciplines • Non-protocolized care • Limited ability for early prognostication (< 72 hours post-arrest) • Differing definitions among studies Resuscitation. 2003;56(3):247-263. Resuscitation. 2006;70(3):404-409. Crit Care Med. 2006;34(7):1865-1873. Resuscitation. 2007;73(1):29-39. Resuscitation. 2007;74(2):227-234.
Survivor Outcomes • Cerebral Performance Category (CPC) • CPC 1: Good cerebral performance • CPC 2: Moderate cerebral disability • Outcomes of CPC 1 or 2 • Adults = 68% • Children = 58% JAMA. 2006;295(1):50-57.
Therapeutic Strategies • General Measures • Monitoring • Hemodynamic Optimization • Oxygenation and Ventilation • Circulatory Support • Managing Underlying Pathology • Therapeutic Hypothermia • Sedation and Neuromuscular Blockade
Therapeutic Strategies • Seizure Control and Prevention • Glucose Control • Neuroprotective Pharmacology • Adrenal Dysfunction Management • Renal Failure Management • Infection Management • AICD Placement • Long-Term Rehabilitation
Therapeutic Hypothermia • 2 RCTs and a meta-analysis showed improved outcome among adults remaining comatose after OOH VF cardiac arrest • Cooling to 32 - 34°C for 12 – 24 hours • 4 studies with historical controls showed benefit after non VF arrest • Observational studies showed benefit with other initial rhythms and in other settings. Crit Care Med. 2005;33(2):414-418 Acta Anaesthesiol Scand. 2006;50(10):1277-1283. Ann Emerg Med. 1997;30(2):146-153. Resuscitation. 2006;69(1):29-32. Crit Care Med. 2006;34(7):1865-1873.
Meta-analysis Alive at hospital discharge with favorable neurologic outcome: Survival Risk Ratio = 1.68 (1.29 – 2.09); NNT = 6 Alive at 6 months with favorable neurologic recovery Survival Risk Ratio = 1.44 (1.11 – 1.76); NNT = 6 Crit Care Med. 2005;33(2):414-418
Therapeutic Hypothermia • Only therapy shown to increase survival following cardiac arrest • Ideal patients, technique, target temperature, duration, and rewarming rate not yet established • Neuroprotection may decrease as the delay in initiation of therapy increases • Time to target temperature = 2 – 8 hours
Therapeutic Hypothermia3 Phase Practical Approach • Induction • Maintenance • Rewarming • If cooling not possible, prevent hyperthermia • Risk highest 48 hours after resuscitation • Poorer neurologic outcome each 1 °C > 37 °C • Treatment: Antipyretics or active cooling
Therapeutic HypothermiaPractical Approach • Induction • “Auto-cooling” or “after-drop” within 1st hour • Ice chilled cold fluids (30 ml/kg NS or LR) • Ice packs (head, neck, axilla, groin) • Shivering prevention (sedation, NMB)
Therapeutic HypothermiaPractical Approach • Maintenance • Continuous temperature feedback • Surface or internal cooling • Cooling blankets or pads • Central Intravascular cooling catheters • Cold wet blankets and ice • Time consuming and less reliable • Cold fluid infusions alone are not adequate • 12 to 24 hours
Therapeutic HypothermiaPractical Approach • Rewarming • Passive rewarming • Active rewarming • Internal or external cooling devices • Other heating systems • Goal 0.25 °C – 0.5 °C per hour • Careful monitoring • Plasma electrolyte concentrations • Hemodynamics
Key Points • Our work is not completed after return of spontaneous circulation • Post-Cardiac Arrest Syndrome represents a complex interaction of underlying pathologies and the body’s response to hypoxia and hypoperfusion • Mild Therapeutic Hypothermia represents a proven therapy that should be provided to comatose, post-cardiac arrest patients • Consider initiation of therapy in the ED for patients remaining > 1 hour after ROSC
Thank you! Questions? silvers.scott@mayo.edu