Uterine Prolapse: Causes, Symptoms, and Management
250 likes | 3.92k Views
Uterine prolapse occurs when the uterus slips out of its normal position into the vagina, causing discomfort and potential health issues. Learn about the degrees, causes, symptoms, and assessment of uterine prolapse in this informative guide.

Uterine Prolapse: Causes, Symptoms, and Management
E N D
Presentation Transcript
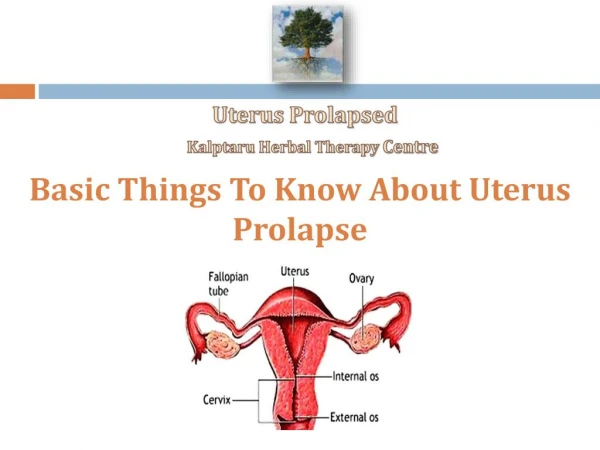
Uterine Prolapse Uterine prolapse ("dropped uterus") is a condition in which a woman's uterus (womb) sags or slips out of its normal position. The uterus may slip enough that it drops partially into the vagina (the birth canal), creating a perceptible lump or bulge. This is called incomplete prolapse. In a more severe case—known as complete prolapse—the uterus slips to such a degree that some of the tissue drops outside of the vagina. Uterus and the cervix lie at right angle of the long axis of the vagina .As the uterus descends, it may pull the vaginal canal and even the bladder and rectum with it. It is the second most common after cystourethrocele (bladder and urethral prolapse).
Prolapse Definition Prolapse literally means "to fall out of place." In medicine, prolapse is a condition where organs, such as the uterus, fall down or slip out of place. It is generally reserved for organs protruding through the vagina, or for the misalignment of the valves of the heart. Uterine prolapse (also called descensus or procidentia) means the uterus has descended from its normal position in the pelvis farther down into the vagina. From:Raafat S Barsoom, (Feb 4,2011) Uterine Prolapse [online] Available from: http://emedicine.medscape.com/article/797295-overview [Accessed:25th Feb 2011]
Displacement of the uterus within the pelvic cavity is classified according to the direction of the displacement which are: • Retroversion - backward tilting of the uterus toward the rectum. • Retroflexion - bending of the uterine corpus in a back manner toward the rectum. • Anterversion - axaggeratedforward tilting of the uterus. • Anterflexion - flexing or folding of the uterine corpus upon itself.
The direction of the displacement normal normal normal Retroversion Retroflexion Anterflexion
Degree of Uterine Prolapse First degree (mild) of uterine prolapse is defined as descent of the uterus to any point in the vagina above the hymen Second degree (moderate) uterine prolapse is defined as descent to the hymen Third degree (severe) - uterine prolapse is defined as descent beyond the hymen
Degree of Uterine Prolapse 2nd degree 1st degree 3rd degree normal
ASSESSMENT • History Patient may complain of one or more of the following: • A feeling of heaviness or pressure in the pelvis • Feeling as if sitting on a small ball or as if something is falling out of the vagina • Pain in the pelvis, abdomen, or lower back • Pain during intercourse • A protrusion of tissue from the vagina • Recurrent urinary tract infections (UTIs) • Unusual or excessive discharge from the vagina • Difficulty with urination, including involuntary loss of urine (incontinence), or urinary frequency or urgency
Physical Examination Performed to exclude the presence of an abdominal or pelvic tumor that may be responsible for the prolapse. Pelvic examination to assess the degree of prolapse is usually performed with the woman either in the left lateral position using a Sims speculum or in a semirecumbent position in the examination chair. Physical findings may be enhanced by having the patient strain during the examination or by having her stand or walk.
Examination in a standing position allows an accurate assessment of the degree of the prolapse. • Stages : • Stage I - Descent of the uterus to any point in the vagina above the level of the hymen • Stage II - Descent to the level of the hymen • Stage III - Descent beyond the hymen • Stage IV - Total eversion or procidentia
ETIOLOGY • The uterus is held in position in the pelvis by muscles, special ligaments, and other tissue. The uterus drops into the vaginal canal when these muscles and connective tissues weaken. • Pregnancy is the main cause of pelvic organ prolapse. It can occur immediately after pregnancy or 30 years later. • Many factors like the weight of the baby, the physical trauma of labor, and birth stresses can strain the pelvic muscles and ligaments.
ETIOLOGY cont. • Normal aging and lack of estrogen hormone after menopause may also cause uterine prolapse. • Chronic cough and obesity increase the pressure on the pelvic floor and may contribute to the prolapse. • Uterine prolapse can also be caused by a pelvic tumor, although this is rare. • Chronic constipation and the pushing associated with it can worsen uterine prolapse.
PATHOPHYSIOLOGY • Displacement or prolapsed of the uterus, bladder, or rectum can be a congenital or an acquired condition. • Congenital tilting or flexion of the uterus is rare. • More commonly, tilting or flexion disorders in which the uterus remains within the pelvic cavity are related to the: • Scarring and inflammation of pelvic inflammatory disease. • Endometriosis • Pregnancy • tumors
PATHOPHYSIOLOGY cont. Downward displacement of the pelvic organs into the vagina result from:
Signs & Symptoms -Women with mild cases of uterine prolapse may have no obvious symptoms. However, as the slipped uterus falls further out of position, it can place pressure on other pelvic organs—such as the bladder or bowel—causing a variety of symptoms, including: Pelvic pressure: a feeling of heaviness or pressure in the pelvis Pelvic pain: discomfort in the pelvis, abdomen or lower back Pain during intercourse A protrusion of tissue from the opening of the vagina Recurrent bladder infections Unusual or excessive discharge from the vagina Constipation Difficulty with urination, including involuntary -loss of urine (female incontinence), or urinary frequency or urgency
Risk Factors • One or more pregnancies and vaginal births • Giving birth to a large baby • Increasing age • Frequent heavy lifting • Chronic coughing • Frequent straining during bowel movements
Causes of Uterine Prolapse -Trauma incurred during the birthing process, particularly with large babies or after a difficult labor and delivery, is one of the main causes of the muscle weakness that leads to uterine prolapse. Reduced muscle tone from aging, as well as lowered amounts of circulating estrogen after menopause, may also form contributing factors in pelvic organ prolapses. In rare circumstances, uterine prolapse may be caused by a tumor in the pelvic cavity. Genetics also may play a role; women of Northern European descent experience a higher incidence of uterine prolapse than do women of Asian and African heritage. Finally, increased intra-abdominal pressure, stemming from such diverse conditions as obesity, chronic lung disease and asthma, can be contributing factors in uterine prolapse.
Screening & Diagnosis -Diagnosing uterine prolapse requires a pelvic examination. You may be referred to a doctor who specializes in conditions affecting the female reproductive tract (gynecologist). The doctor will ask about your medical history, including how many pregnancies and vaginal deliveries you've had. He or she will perform a complete pelvic examination to check for signs of uterine prolapse. You may be examined while lying down and also while standing. Sometimes imaging tests, such as ultrasound or magnetic resonance imaging (MRI), might be performed to further evaluate the uterine prolapse. 7
Treatment -Losing weight, stopping smoking and getting proper treatment for contributing medical problems, such as lung disease, may slow the progression of uterine prolapse. -If you have very mild uterine prolapse, either without symptoms or with symptoms that aren't highly bothersome, no treatment is necessary. However, without treatment, you may continue to lose uterine support, which could require future treatment. Non-Surgical Options Surgical Options Hysterectomy is a way of treating problems that affect the uterus. Many conditions can be cured with hysterectomy. Because it is major surgery, you may want to explore other treatment options first. For conditions that have not responded to other treatments, a hysterectomy may be the best choice. You should be fully informed of all options before you decide.
Screening & Diagnosis -Diagnosing uterine prolapse requires a pelvic examination. You may be referred to a doctor who specializes in conditions affecting the female reproductive tract (gynecologist). The doctor will ask about your medical history, including how many pregnancies and vaginal deliveries you've had. He or she will perform a complete pelvic examination to check for signs of uterine prolapse. You may be examined while lying down and also while standing. Sometimes imaging tests, such as ultrasound or magnetic resonance imaging (MRI), might be performed to further evaluate the uterine prolapse. 7