Download

1 / 37
440 likes | 628 Views
Learn to define, classify, and treat genital prolapse, discussing anatomy, causes, and treatment options. Includes a clinical case for practical application.

E N D
OBJECTIVES OF THE LECTURE • At the end of this lecture: • The student should be able to • Define prolapse. • Classify prolapse using a simple conventional system. • Understand the anatomical basis of genital prolapse. • Discuss the aetiological factors associated with genital prolapse. • Understand the clinical presentation of genital prolapse. • Initiate appropriate investigations in a patient with genital prolapse. • Understand the basis of non-surgical and surgical treatment of genital prolapse. • Offer appropriate counselling for prophylaxis of genital prolapse. • Should be able to diagnose and offer basic advise on the treatment and prophylaxis of genital prolapse.
CLINICAL CASE A 56 year old para 6+2+4+7 who attained menopause 2 years ago presented in the clinic with the complaints of “something” protruding through the vagina for about 8 months. In the last two months she has had some backache, a troublesome cough and more recently she had some difficulties with her “water” control. Discuss the management of this case
"CLINICAL CASE" NOT PROBLEM MAIN PROBLEMS AGE - 56 years PARITY: 6+2+4+7 MAIN SYMPTOMS: - “Something” protruding through the vagina - 8 months - Back ache - Cough troublesome - “Water” control
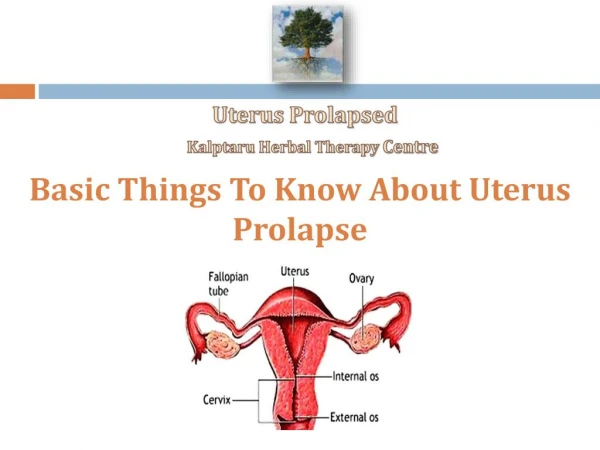
DEFINITION Prolapse is defined as:- Herniation or protrusion or descent of one or more of the pelvic viscera through the vagina as a result of a defect in the pelvic floor due to damage or weakness. Simply put-one of the pelvic viscera “falls through” or “protrudes” through the vagina as a “mass” Which pelvic viscera / organs are involved? Urethra, Bladder Uterus Bowels, Rectum.
Urethrocele (Urethrocoele) Sagging of urethra and the associated anterior vaginal wall into the vaginal lumen Cystocele (Cystocoele) Herniation or protrusion of the bladder into the vaginal canal Usually involves anterior vaginal wall , May be mild, moderate or severe (or small, average, Large). May co-exist with prolapse of the urethra when the terminology should be Cysto-urethrocele.
Uterovaginal prolapse Descent of the cervix and uterus along the axis of the vaginal canal. In severe cases, the vagina is everted and the cervix occupies a position outside vagina. Degree of prolapse depends on location of cervix / uterus in vagina. Retroversion of uterus- A NEW CLASSIFICATION OF THE VARIOUS STAGES OF UTEROVAGINAL PROLAPSE EXISTS BUT WE SHALL USE THE WELL ESTABLISHED STAGING
First Degree Cervix descends within the vagina but does not reach introitus Second Degree Descent of the cervix to the introitus Cervix may descend beyond introitus with straining but return to introitus later Third Degree (Procidentia) Descent of the cervix beyond the introitus (without straining i.e. at rest) In some cases – uterus lies completely outside vagina-walls of vagina everted
Vault Prolapse Hernation usually of bowels through vaginal vault after hysterectomy. Enterocele (Enterocoele) Hernation / out pouching / protrusion of peritoneum over pouch of Douglas (through posterior vaginal fornix) Sca usually contains loops of bowl. Rectocele (Rectocoele) Sagging or protrusion of rectum into the vagina. May be mild, moderate or severe (small, Average, Large).
Note • Utero-vaginal prolapse which technically applies to prolapse of the uterus is frequently (almost always) associated with • Prolapse of organs through the anterior vaginal wall • - Urethrocele / Cystocele • Prolapse of organs through the pouch of Douglas and posterior vaginal wall • - Enterocele / Rectocele • Various combinations of above entities occur in different patients • Laxity of the Introitus
INCIDENCE Occurs World wide. Variation with age / Parity Increase with age Increase with parity More common amongst whites Less common amongst Asians, Arabs, Afro Americans. Africans About 50% of patients are parous Women have some degree of prolapse. About 2% Nulliparous women may have symptomatic prolapse.
ANATOMY OF THE PELVIC FLOOR AND SUPPORT OF THE PELVIC ORGANS Muscles of the pelvic floor * Levator Ani Muscles The Endopelvic fascia * Pubocervical fascia * Transverse cervical Ligaments * (Cardinal Ligaments) * Utero-sacral Ligaments * Recto-vaginal fascia Round Ligaments of the uterus
AETIOLOGY OF PROLAPSE • Congenital Weakness of pelvic floor • - Rather less common • 2. Congenital Elongation of the cervix – Rare • 3. Race - Connective Tissue structure / Disorder • - Fibrous Tissue formation after injury • - Work Ethics / Physical Exertion • 4. Age -
5. The role of pregnancy / Delivery • * Parity • * Prolonged labour • * Feto-pelvic disproportion • * Difficult vaginal / Instrumental Deliveries • (Forceps / Ventouse) • * Traumatic Lacerations • * Episiotomy • The role of hormones • * Estrogens and postmenopausal atrophy
Precipitating Factors-Increased Abdominal pressure • * Chronic cough • * Intra abdominal Masses / Tumours • * Ascites • * Chronic constipation with repeated straining at stool • * Tight - fitting corsets • * Excessive physical exertion / lifting of heavy objects • * Obesity
Previous surgery – May cause vault prolapse or enterocele • * Abdominal Hysterectomy • * Vaginal Hysterectomy • * Manchester operation • (failure to recognise enterocele at the time of initial surgery) • * Burch colposuspension (May leave posterior vaginal defect enterocele)
CLINICAL PRESENTATION • Symptoms – Varied depending on: • a. Type of prolapse • b. Degree / severity • Most frequent symptom: • “Something coming down the vagina” • “Mass protruding from the vagina” • “Mass / Lump in the vagina” • “Pressure / fullness in the vagina” • “Worse with strain / exertion” • “Worse at the end of the day” • “ Relieved with bed rest” • “Mild symptoms at beginning of day”
B. Other symptoms include • Vaginal Discharge • Vaginal bleeding • (Decubitus ulceration of Cx-dependent protruding area) • Dragging sensation / Abdominal pain • Backache • Dyspareunia
C. Problems with Micturition [Urethrocele] • [Cystocele severity] • Frequency • Urgency • Stress Incontinence • Difficulty with initiating micturition • Feeling of incomplete emptying of bladder • (Patient may have to push through the anterior vaginal wall to assist with micturition) • Dysuria: symptoms of U.T.I • With severe prolapse (procidentia) With severe prolapse (Procidentia Hydro-ureter Hydro-Nephrosis. U.T.I
D. Bowel difficulties: [Rectocele] • Constipation • Incomplete evacuation of rectum • (assistance with pressure on posterior vaginal wall to assist bowel evacuation) • E. Precipitation Factors: • * Chronic cough • * Ascites • * Abdominal / Pelvic Tumours
Signs: • General Examination. • Blood pressure • Heart sounds • Respiratory system • Abdomen – Masses / Ascites
Vaginal Examination • A. Inspection • Stress Incontinence (If bladder empty, repeat examination after 1 hour and encourage patient to drink) • B. Speculum Examination • Sim’s position / Lateral position • Sim’s speculum • Anterior vaginal wall • Posterior vaginal wall • C. Digital Examination
Symptoms Frequency • Protrusion >90% • Pressure >90% • Impaired Coitus 37% • Difficulty voiding 33% • Urinary Incontinence 33% • Difficulty walking 25% • Difficulty Defaecating 25% • Pelvic pain 17% • Urinary frequency / urgency 14% • Nausea 10% • Low back pain 10% • Mucosal Irritation / Discharge 10% • Addision et al 1988
INVESTIGATIONS • Sickling / Hb Electrophoresis • Liver Function Tests • Renal Function Test • Fasting Blood sugar • Mid stream Urine-Protein / Sugar • Microscopy, Culture and Sensitivity • ECG (in elderly patients) Chest X ray (chronic cough) • Special • Stress Incontinence – Urodynamic studies • IVU – (Severe prolapse) Abdominal mass • CT Scan – (Abdominal Masses / Tumour / Ascites / ) MRI
Treatment • A. General • Health of patient-Respiratory • Disorders / Heavy smoking • Estrogen Therapy in menopausal patients • Physiotherapy • Pelvic floor exercises • Treat U.T.I if detected
Non - Surgical • (a) Temporary treatment • i In pregnancy • ii While awaiting surgery • (b) Long term treatment • i Frail / Elderly patient • ii Patient unfit for Anaesthesia • iii Unfit for surgery • iv Unwilling for surgery • Silicone Ring Pessary – Different sizes • - Main stay • Appropriate size of pessary • Change every 306 months • Regular check – up • Probable side Effects –vaginal discharge • Coital Problems • (with Rubber Pessaries) Ulceration / Cancer Vaginal bleeding.
C. Surgical • Depends on • a. Type of prolapse • b. Age of patient • c. Desire for future reproduction • d. Coital activity • Surgery is the definitive cure for all forms of prolapse • There are complications after various surgical operations
1. Cystourethrocele Anterior Colporrlaphy Modify if stress incontinence present. TOT/TVT Complications: Haemorrhage Haemorrhage Vesico-Vaginal fistula Retention of urine / UTI Post operation * Dyspareunia * Recurrence
2. Rectocele *Posterior Colporrhapy • *Posterior Colpo-perineorrhapy • ( Where perineum is deficient) • *Complications – Haemorrhage • Recto-vaginal fistula • * Dyspareunia
Uterovaginal Prolapse Young patient / Sexually Active / Wants more children Manchester Type operation * Dilation and Curettage * Amputation of cervix * Shortening of cardinal ligaments and Approximation in front of cervix. Forthergill and Stumdorf stitches Combine with Anterior Colporrhaphy Posterior colpo-perineorrhaphy Repair of Enterocele
Complications of Manchester Operation: - Dyspareunia - 2° Infertility-cervical factor - Recurrence of prolapse Mainly Obstetric - Recurrent abortion-Mid trimester - Premature labour - Cervical dystocia - Obstructed labour Cervical laceration Delivery after Manchester Operation Some authors advocate Tubal Ligation with Manchester operation Delivery by Elective C/S Vaginal delivery Shorten second stage (Easy Forceps/Ventouse)
3.2.1. Utero-vaginal prolapse [1° -2° Degree Prolapse] • Sexually active / Family size complete • EITHER • Manchester Type operation • With anterior colporrhaphy and as indicated • Posterior colpoperineorrhaphy • Repair of enterocele • OR • Vaginal Hysterectomy • AND • Pelvic repair (as indicated) • [Anterior colporrhaphy/posterior colpo perineorrhaphy] • 3.2.2 Utero-vaginal Prolapse • Elderly patients (post Menopause) • All others-especially when procidentia present • Vaginal hysterectomy and • Pelvic floor repair
4. LE FORT’S Operation • Rarely performed Nowadays • Closure of vagina • Colpocliesis • In frail elderly patients
Complications of vaginal Hysterectomy Haemorrhage Ureteric Injury Bowel Injury Pelvic Haematoma Pelvic Absess Dyspareunia Delayed Vault Prolapse OTHER SURGICAL OPERATIONS
d. Prophylaxis (Prevention) • Improvement in general health • Good Obstetric care • * Posnatal pelvic floor exercises • * Prevent prolonged labour • * Shorten second stage
* Prevent difficult deliveries • * Prevent lacerationof the genital tract • * Proper Repair of Episiotomy • * MORE CAESAREAN SECTIONS! • Reduce parity • Hormone Replacement Therapy • (Menopause)
Write short notes on The common symptoms of genital prolapse. The complications of vaginal hysterectomy. The complications of anterior colporhaphy. The aetiological factors that may predispose to uterovaginal prolapse. Prevention of uterovaginal prolapse. QUESTIONS????