Download

1 / 40
420 likes | 607 Views
Cutting among Adolescents aka Self-injury. Zena Edwards Michael Varady June 10, 2005. What do these people have in common?. Angelina Jolie Christina Ricci Courtney Love Princess Diana. Promoting The Cutting Culture. Websites-“Blood Red” -“Razor Blade Kisses” -“The Cutting World”

E N D
Cutting among Adolescentsaka Self-injury Zena Edwards Michael Varady June 10, 2005
What do these people have in common? • Angelina Jolie • Christina Ricci • Courtney Love • Princess Diana
Promoting The Cutting Culture • Websites-“Blood Red” -“Razor Blade Kisses” -“The Cutting World” • Films- “Thirteen” • Genre of music- “emo”
It is NOT self-injury if your primary purpose is… • Sexual pleasure • Body decoration • Spiritual enlightenment via ritual • Fitting in or being cool • Attempting suicide
Self-inflicted violence Self-mutilation Self-abuse Self-injury Self-harm Parasuicide Delicate cutting Terms for self-injury
Knives Razors Glass Pins Any sharp object Burning (35%) Cutting, scratching (72%) Hitting your body with an object or your fists (35%) Hitting a heavy object (like a wall) Picking at skin or scab until it bleeds (22%) Biting yourself Pulling your hair out (10%) Inserting objects in body openings Bruising or breaking bones (8%) Instruments/Methods
Areas most typically injured • Arms and wrists • Legs • Abdomen • Head • Chest • Genitals
What do self-Injurers say about …..Why they do it? 'to run away from my feelings' 'to feel pain on the outside instead of the inside' 'to cope with my feelings' 'to express my anger toward myself' 'to feel like I'm real' 'to turn off emotions and hide from reality' 'to tell people that I need help' 'to get people's attention' 'to tell people I need to be in hospital' 'to get people to care about me' 'to make other people feel guilty' 'to drive people away' 'to get away from stress and responsibility' 'to manipulate situations or people'
Definition • Self-injury is “the act of attempting to alter a mood state by inflicting physical harm serious enough to cause tissue damage to the body.” • Usually deliberate, repetitive, impulsive, and non-lethal • “Tissue damage” refers to damage that tears, bruises, or burns the skin– something that causes bleeding or marks that don’t go away in a few minutes.
DSM IV-TR • No formal classification • Self-injury behavior is seen in connection with a number of diagnosis • Borderline Personality Disorder • Depression • Eating Disorders (anorexia and bulimia) • Obsessive-Compulsive Disorders (OCD) • Post-Traumatic Stress Disorder (PTSD) • Dissociative Disorders • Anxiety and Panic Disorders • Impulse Disorder Not Otherwise Specified
Overall picture of Self-injurer • Person who strongly dislikes/invalidates oneself, low self-esteem • Are hypersensitive to rejection • Chronically angry, usually at themselves, tend to suppress their anger, high levels of aggressive feelings which they disapprove of strongly and which are suppressed or directed inward • More impulsive, lacking in impulse control, act in accordance with their mood of the moment • Tend not to plan for future
Picture cont… • Depressed and suicidal/self-destructive • Suffer chronic anxiety • Tend toward irritability • Do not see themselves as skilled in coping • Do not have a flexible repertoire of coping skills • Do not think they have much control over how/whether they cope with life • Tend to be avoidant • Do not see themselves as empowered
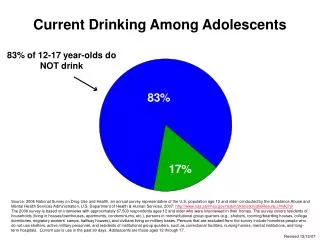
Incident and Onset • 12% to 14% of adolescents reported self-injury behavior • 40% to 61% in adolescent inpatient settings (Ross & Heath, 2002) • Higher proportion of females (64%) than males (36%) • 750 per 100,000- general population • Typical onset-puberty • Persist for five to ten years or longer
Key Emotional Motivators • Anger/frustration/rage- (68%) • Fear- (36%) • Self-hatred- (32%) • Desperation/despair- (27%)
Warning Signs • Unexplained frequent injuries, including cuts and burns • Wearing long pants and sleeves in warm weather • Low self-esteem • Difficulty handling feelings • Poor functioning at work, school or home • Relationship problems
Predictors • Past trauma/invalidation • Van der Kolk, Perry, and Herman (1991) • Exposure to physical or sexual abuse • Physical or emotional neglect • Chaotic family conditions during childhood, latency, and adolescence • Invalidation independent of abuse • Linehan (1993a) • “invalidating environments” –one in which communication of private experiences is met by erratic, inappropriate, or extreme responses
Invalidation cont. • Two primary characteristics • Tells the individual that they are wrong both in their description and analysis of of their own experiences, especially as to what is causing emotions, beliefs, and actions • Attributes one’s experiences to socially unacceptable characteristics or personality traits
Forms of invalidation • “You’re angry but you just won’t admit it” • “You say no but you mean yes, I know” • You really did do (something you in truth hadn’t). Stop lying” • “You’re being hypersensitive” • “You’re just lazy” • “I won’t let you manipulate me like that” • “Cheer up. Snap out of it. You can get over this” • “If you’d just look on the bright side and stop being a pessimist…” • “You’re just not trying hard enough” • “I’ll give you something to cry about”
Predictors • Biological/Neurochemistry • Carlson (1986) • Reduced levels of serotonin & increase in endorphin rush • Decreases in necessary brain neurotransmitters • Behaviorists • Operant conditioning • Positively reinforced by getting attention and repeat self-harming act • The sensory stimulation associated with self-harm serves as a positive reinforcer and stimulus for further abuse • Sensory Contingencies • Attempting to mediate levels of sensory arousal (increase or mask sensory input) • Release of physiological tension/arousal
Therapeutic Approaches • Dialectical Behavioral Therapy (BPD) • Interpersonal Group Therapy (BPD) • The CPTSD Approach (non-BPD) • Rational-Emotive Therapy (non-BPD) • Psychopharmacological • Hypnosis and relaxation • Hospital-based treatment
Dialectical Behavioral Therapy Dialectical Behavioral Therapy (DBT) consists of two parts: • Once-weekly psychotherapy sessions in which a particular problematic behavior or event from the past week is explored in detail, beginning with the chain of events leading up to it, going through alternative solutions that might have been used, and examining what kept the client from using more adaptive solutions to the problem:Both between and during sessions, the therapist actively teaches and reinforces adaptive behaviors, especially as they occur within the therapeutic relationship. • Weekly 2.5-hour group therapy sessions in which interpersonal effectiveness, distress tolerance/reality acceptance skills, emotion regulation, and mindfulness skills are taught. Group therapists are not available over the phone between sessions; they refer patients in crisis to the individual therapist.
Interpersonal Group Therapy • time-limited group psychotherapy • a Rogerian, client-centered facilitation style. Group disagreements and disappointments with the therapists or other group members are worked out within the group by clients, with the therapists intervening only when the process of therapy seems to be getting off-track ("derailing"). • Therapist interventions are intended to be tentative, exploratory, indirect, and neutral. Two-sided commentary, reiteration/paraphrasing, reflecting doubt/confusion, answering of enquiries, and supportive statements are part of the IPG model.
The CPTSD Approach • three stages: establishing safety, remembrance and mourning for what was lost, and reconnecting to society. • name the problem- acknowledging the trauma and its past and present effects, both mental and physical. • restore a sense of control to the client. • establishing a safe environment: setting up support networks of caring people, helping the client to protect him/herself from any physical danger they may face, and developing a plan for dealing with for future protection, one that takes into account any self-destructive behaviors the client engages in. • Even after these steps are complete, the trauma may never be fully resolved; recovery is to be a lifelong process. However, at this point, it becomes on of many factors in a client's life and not the dominant one.
Rational-Emotive Therapy • Doesn't directly address self-harm as an issue, its precepts can be helpful in controlling the sometimes uncontrollable rage self-injurers feel. • Rational-Emotive therapy was developed by Albert Ellis • your feelings don't control your thoughts -- your thoughts control your feelings. • Negative emotions are not inevitable, but come about as the result of patterns of thinking we've laid down over the years. • If we can learn to rethink the situations, we can learn to control negative emotions.
Psychopharmacological Approaches • Neurotransmitters are chemicals used to transmit messages in the brain. • Different neurotransmitter receptors affect different bodily functions. These receptors are involved in regulating emotion, mood, impulsivity, aggression, digestion, smooth muscle relaxation, and sexual behavior, among other functions. • Three sorts of neurotransmitters have been of concern to scientists studying self-injurious behavior: serotonin, dopamine, and endorphins. The strongest evidence so far points to serotonergic deficits -- the brain does not have enough serotonin available for use. • The theory is that self-mutilation releases endorphins and over time, the body becomes addicted to these pain-relieving neurotransmitters. The impulse to self-injure arises from a craving for endorphins.
Psychopharmacological drugs • Probably the most investigated drugs for SIB are naltrexone and naloxone, opiate antagonists. • The new class of atypical neuroleptics, which tend to bind to dopamine and serotonin receptors, seem to show some promise in treating SIB as well. • Clozapine has been reported to reduce SIB in personality disordered subjects • These drugs can also have troublesome side effects -- patients on clozapine, for example, require weekly blood tests because of the risk of white-blood-cell abnormalities.
Hypnosis and relaxation • Hypnotic relaxation techniques have apparently been used, with some success, as an adjunct to therapy. • three types of hypnosis: • Breath counting: the patient is led into a trance and instructed to notice her breathing, counting each deep slow breath. • Positive imagery: the patient is put into a trance state and instructed to visualize herself in a calm, pleasant, relaxing place doing something she enjoys. This image is held for a while. • Affect bridge: after trance is achieved, the patient is asked to use the current unpleasant feelings to remember other times in his life when he's felt this way. Memories that are too distressing to talk about in a normal state are sometimes speakable in a trance state.
Hospital-based treatment • SAFE Alternatives (1-800-DONTCUT) is an inpatient program specifically for self-injurers located at MacNeal Hospital in a Chicago suburb • The program combines milieu therapy, cognitive-behavioral therapies, and group and individual exercises to help patients gain an awareness of why they hurt themselves and how to stop. • They claim to be the only inpatient unit for self-injurers in the U.S. • The Sanctuary at Friends' Hospital in Philadelphia is an inpatient unit for trauma survivors that is aware of the special needs of self-injurers and takes them into account in its treatment program. • Butler Hospital in Rhode Island offers a partial hospitalization program that uses dialectical behavioral therapy to treat a diverse patient population of self-injurers.
Helpful Unconditional acceptance and compassion A non-judgmental attitude Trust and reliability Kindness, caring, honesty Empathy, warmth, genuineness Active listening Being treated with firmness/gentleness Confidential and safe setting Being trusted to take care of one’s own wounds support and space to explore difficult issues Gaining self-awareness and insight into the thought processes Revealing scars for the first time Being listened to, believed, taken seriously, feeling understood Feeling safe to cry and express feelings Developing healthier coping strategies Unhelpful A dictatorial, arrogant and judgmental approach Denying the problem exists Lack of continuity Deeply engrained issues not being addressed Sympathy Personal prejudice Not being heard Preconceived ideas/stereotyping Being left alone to cope with the aftermath “No self-harming” contracts Being “labeled” Too much too soon-probing into where a client is not ready to go What Helps/Hinders healing from self-injury
What is a School Counselor to do? • Primary goal- create a safe environment • Foster a strong alliance with the student • Emphasis on structure, consistency, and predictability that is modeled in counseling • Developing a detailed safety plan with the student that emphasizes the students’ taking responsibility for behaviors • identifying self-injury triggers, physical cues, and reducers related to self-injury • Exploring safe people/places to go when wanting to self-injure • Deliberate avoidance of objects that can be used to self-injure
School Counselor cont… • Techniques to help students manage self-injurious impulses: • Increasing feeling awareness and recognition • Increasing coping skills to be used in managing feelings • Encouraging the use of self-soothing techniques such as relaxation exercises • Encouraging the use of safe places
Cessation factors of self-injury behavior • Developing an ability to identify and express feelings verbally • Learning to use behavioral alternatives to self-injury • Development of impulse control • Sense of control in managing the self-injurious behaviors “Self-harm is rarely done when others are nearby”
Caveat for School Counselors • Possibility of accidental death as a result of damage inflicted on the body • Important to assess a student’s self-injury • Severity of the behaviors (severe & chronic) • Possible medical complications (infections) • Issues related to suicide • Assessment of depression, helplessness, hopelessness • Suicide ideation, plan and intent, preparation and access to means, past attempts • Social support • Family history • Recent stressors
Referral Issues • The role of the school counselor is intervention and prevention NOT diagnosis and treatment • Make a referral for inpatient or out-patient treatment • Be knowledgeable of practitioners and treatment centers that have specific training in the management of self-injury • Continue to play a role in the student’s treatment process if appropriate • Safe person the student can talk to • Arranging home tutoring/collaborating with the educational tutor at the residential center or hospital • Advocate for students • Faculty in-services • Parenting groups • Classroom guidance on self-injury
Can I trust you with my pain? To treat it with kindness and respect? To listen to it, So I can speak the unspoken? If I entrust you with my grief, Will you help me take care of it? Console it? Soothe it? Make it feel safe? Will you accept it as a gift to be protected? I feel my need and I fear it, As I fear all that I do not understand, Yet I ask you to be with me, For I am tired of walking alone Will you help me catch my tears As the floodgates open? Swim with me into the unknown? Save me from drowning in my sorrow? If I take the risk and end the drought, Will you leave me alone and sodden after the storm? Will you reach for your umbrella, And just walk away? Be with me please Source: Healing the Hurt Within: Understand and relieve the Suffering behind self-behavior, Jan Sutton
References Alderman, T. (2000). Helping those who hurt themselves. The Prevention Researcher, 7, 4. Froeschle, J. & Moyer, M. (2004). Just cut it out:legal and ethical challenges in counseling students who self-mutilate. Professional School Counseling, 7 (4), 231-235 HealthyPlace. Who self-injures: Psychological characteristics common in self-injurers. Retrieved June 3, 2005 from www.healthyplace.com/communities/self_injury/ S.A.F.E. Alternatives. SI Facts. www.safe-alternatives.com/sifacts.html SIARI. Self-injury and Related Issues. www.siari.co.uk Stone, J.A. & Sias, S.M. (2003). Self-injurious behavior: A bi-modal treatment approach to working with adolescent females. Journal of Mental Health Counseling, 25 (2), 112-125. Sutton, J. & Martinson, D. (2005). Self-injury: You are NOT the only one. Retrieved June 3, 2005 from http:crystal.palace.net/~llama/selfinjury/ Suyemoto, K.L. & Kountz, X. (2000). Self-mutilation. The Prevention Researcher, 7(4), 1-2. White-Kress, V.E., Gibson, D.M. & Reynolds, C.A. (2004). Adolescents who self- injure: Implications and strategies for school counselors. Professional School Counseling,7 (3), 195-201. Whitmarsh, L., Rosencrance, J., Lynch, M. & Mullette, J. (nd.). Adlolescent self-multilation: Research review and case presentations. Retrieved June 3, 2005 from www.angelfire.com/journal2/njca/Whitmarsh.html.