Smallpox Eradication: Lessons, Challenges & Future Implications
Learn about the history of the smallpox vaccine, its eradication, complications, and the global vaccination campaign. Understand the risks, benefits, and the role of medical care in preventing a smallpox resurgence.


Smallpox Eradication: Lessons, Challenges & Future Implications
E N D
Presentation Transcript
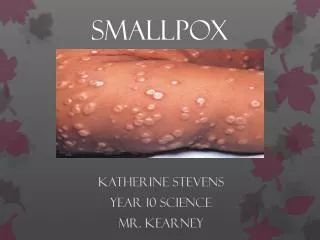
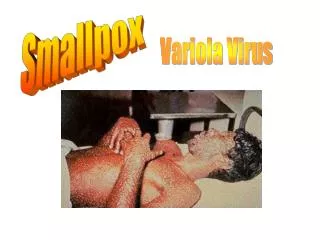
Smallpox Lessons Learned and Future Challenges
Why Smallpox Bioterrorism? • Stable aerosol Virus • Easy to Produce • Infectious at low doses • Human to human transmission • 10 to 12 day incubation period • High mortality rate (30%)
Co-Evolution • Smallpox infects humans only • Could not survive until agriculture • No non-human reservoir • If at any point no one in the world is infected, then the disease is eradicated • Infected persons who survive are immune, allowing communities to rebuild after epidemics
Small Pox Vaccine History • 1000 AD - China, deliberate inoculation of smallpox into skin or nares resulting in less severe smallpox infection. Vaccinees could still transmit smallpox • 1796 - Edward Jenner demonstrated that skin inoculation of cowpox virus provided protection against smallpox infection • 1805 - Italy, first use of smallpox vaccine manufactured on calf flank • 1864 - Widespread recognition of utility of calf flank smallpox vaccine • 1940’s - Development of commercial process for freeze-dried vaccine production (Collier)
How Vaccination WorksHerd Immunity • Smallpox Spreads to the Non-immune • Immunization Slows the Spread Dramatically • Epidemics Die Out Naturally • Herd Immunity Protects the Unimmunized
Smallpox Vaccine • Live Virus Vaccine (Vaccinia Virus) • Not Cowpox, Might be Extinct Horsepox • Must be Infected to be Immune • Crude Preparation We Have Now • Prepared from the skin of infected calves • Filtered, Cleaned (some), and Freeze-dried • New Vaccine is Clean, but still Live
Complications of Vaccination • Local Lesion • Can be Spread on the Body and to Others • Progressive (Disseminated) Vaccina • Deadly Like Smallpox, but Less Contagious • Encephalitis • Heart Disease?
Historic Probability of Injury • Small Risk from Bacterial and Viral Contaminants • Small Risk of Allergic Reaction • 35 Years Ago • 5.6M New and 8.6M Revaccinations a Year • 9 deaths, 12 encephalitis/30-40% permanent • Death or Severe Permanent Injury - 1/1,000,000 • Mostly among immunsupressed persons
Global Eradication Program • 1950 - Pan American Sanitary Organization initiated hemisphere-wide eradication program • 1967 - Following USSR proposal (1958) WHO initiated Global Eradication Program • Based on Ring Immunization • Vaccinate All Contacts and their Contacts • Isolate Contacts for Incubation Period • Involuntary - Ignore Revisionist History • 1977 - Oct. 26, 1977 last known naturally occurring smallpox case recorded in Somalia • 1980 - WHO announced world-wide eradication
Eradication Ended Vaccinations • Cost Benefit Analysis • Vaccine was Very Cheap • Program Administration was Expensive • Risks of Vaccine Were Seen as Outweighing Benefits • Restatement of Torts 2nd - Products Liability • Stopped in the 1970s • Immunity Declines with Time
Post Eradication • 50%+ in the US have not been vaccinated • Many fewer have been vaccinated in Africa • Immunity fades over time • Everyone is probably susceptible • Perhaps enough protection to reduce the severity of the disease
Role of Medical Care • Smallpox • Can Reduce Mortality with Medical Care • Huge Risk of Spreading Infection to Others • Very Sick Patients - Lots of Resources • Cannot Treat Mass Casualties • Vaccinia • VIG - more will have to be made • Less sick patients - longer time
The Danger of Synchronous Infection • The whole world may be like Hawaii before the first sailors • If everyone gets sick at the same time, even non-fatal diseases such as measles become fatal • A massive smallpox epidemic would be a national security threat • Is a massive epidemic possible?
Smallpox Vaccination Campaign Fall 2002 - Spring 2003
Why Did White House Wait so Long? • Key year for bioterrorism – 1993 • Credible information that the Soviet Union had tons of smallpox virus it could not account for • CIA did not tell CDC • Still Debating Destruction of the Virus in 1999 • Should have started on a new vaccine • Should have worked out a vaccination program
Vaccinating the Military • Required of Combat Ready Troops • Combat ready personnel are medically screened and discharged if they have conditions that would complicate vaccination • All are young and healthy • Not a good control group
Vaccinating Health Care Workers • All ages • Many have chronic diseases that compromise the immune system or otherwise predispose to complications • Have not been medically screened • ADA makes medical screening legally questionable • Political concerns make it impossible
CDC Plan • Voluntary vaccinations • No screening or medical records review • Self-deferral
Problems in the CDC Plan • Conflicting information on removing vaccinated workers from the workplace • No focus on who should be vaccinated - random volunteers do not produce a coherent emergency team • Assumed patients would walk into the hospital • Ignored Securing ERs to prevent this • No attention paid to hospital and worker concerns
Liability for Primary Vaccine Injuries • Informed Consent • Was the Patient Warned of the Risk? • Is it 1/1,000,000 or is it 1/10 for the Immunosuppressed? • Negligent Screening • Is it reasonable to rely on self-screening when the clinical trials demanded medical testing and records review?
Liability for Secondary Spread • Spread to Family Members • Is a Warning to the Vaccinee Enough? • Should there be investigation of the health status of family members? • Spread to Patients by Health Care Providers • Should Vaccinated Persons be in the Workplace while Healing? • Should Patients be Warned?
Employment Discrimination Issues • What Happens When Health Care Providers and Others Refuse Vaccination? • What if they Cannot be Immunized? • Must they be Removed from Emergency Preparedness Teams? • What about Other Workplace Sanctions?
Costs to Hospitals and Workers • Is a vaccine injury a worker's compensation injury? • Should be, but many comp carriers baulked at assuring they would pay • Who pays for secondary spread injuries? • Who pays for time off work and replacing workers? • Does the worker have to take sick leave?
Homeland Security Act Solution • "For purposes of this section, and subject to other provisions of this subsection, a covered person shall be deemed to be an employee of the Public Health Service with respect to liability arising out of administration of a covered countermeasure against smallpox to an individual during the effective period of a declaration by the Secretary under paragraph (2)(A)."
What Triggers This? • Secretary of HHS Must Make a Declaration • Must Specify the Covered Actions • Immunity Only Extends to Covered Use of Vaccine • Does Not Apply to Unauthorized Use or Blackmarket • Includes People and Institutions
What is Excluded? • Probably Worker’s Comp • Not a Liability Claim • If Included, then the Injured Worker has no Compensation • Black-market and direct person to person inoculation • Only injuries, not costs of lost time and other hospital costs
Effect on Injured Workers, Their Families, and Patients • No compensation beyond comp • Questions about whether comp would pay • Might have to use vacation and sick leave • Smallpox compensation act was eventually passed but not implemented and is too limited
The Real ProblemLack of Information • What is the real risk of complications? • Never clarified the risk to immunosuppressed persons • Why now? • Has something really changed? • Is this just Swine Flu all over again?
The End Result • Less than 35,000 vaccinated out of a target of 500,000 • Many of those were reservists who were vaccinated outside the hospital setting • Smallpox vaccination has been discredited
Modeling Smallpox and the CDC, Post Smallpox Immunization Campaign
The Dark Winter Model • Johns Hopkins Model - 2001 • Simulation for high level government officials • Assumed terrorists infected 1000 persons in several cities • Within a few simulated months, all vaccine was gone, 1,000,000 people where dead, and the epidemic was raging out of control
Response to the Dark Winter Model • Koopman – worked in the eradication campaign • “Smallpox is a barely contagious and slow-spreading infection.” • Lane – ex-CDC smallpox unit director • Dark Winter was “silly.” “There’s no way that’s going to happen.”
Decomposing the Models – Common Factors • Population at risk • Initial seed • Transmission rate • Control measures under study
Population at Risk • Total number of people • Compartments - how much mixing? • Immunization status • Most assume 100% are susceptible • Increasing the % of persons immune to smallpox • Reduces the number of susceptibles • Dilutes the pool, reducing rate of spread
Transmission Rate • Mixing Coefficient X Contact Efficiency • Mixing Coefficient • The number of susceptible persons an index case comes in contact with • Contact Efficiency (Infectivity) • Probably of transmission from a given contact • Can be varied based on the type of contact
Transmission Rate is the Key • < 1 - epidemic dies out on its own • 1 - 3 - moves slowly and can be controlled without major disruption • > 5 - fast moving, massive intervention needed for control • > 10 - overwhelms the system - Dark Winter
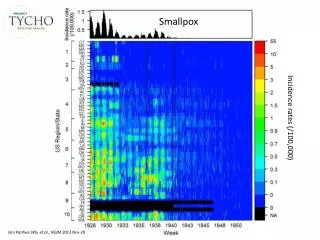
What is the Data on Transmission Rate? • Appendix I • http://whqlibdoc.who.int/smallpox/9241561106_chp23.pdf • This is all the data that exists • The data is limited because of control efforts • This data supports any choice between 1 and 10
Dark Winter - Risk of 10 • Can only be prevented by the reinstituting routine smallpox immunization • Terrible parameters for policy making • Huge risk if there is an outbreak • Low probability of an outbreak
Kaplan - Risk of 5 • Mass immunization on case detection • Best to pre-immunize health care workers
Metzler/CDC - Risk of 2-3 • Contact tracing and ring immunization • Trace each case and immunize contacts • Immunize contacts of contacts • Takes a long time to get the last case
Reinstituting Routine Vaccinations • We cannot even get people to get flu shots, which is perfectly safe • No chance that any significant number of people will get the smallpox vaccine after the failure of the campaign to vaccinate health care workers • Would require a massive federal vaccine compensation program
Mass Vaccinations Post-Outbreak • Pros • Limits the duration of the outbreak to the time necessary to do the immunizations, could be two weeks with good organization • Eliminates the chance of breakout • Cons • Lots of complications and deaths from the vaccine • Requires massive changes in federal vaccine plans
Contract Tracing and Ring Immunizations • Pros • Limits the vaccine complications • Does not require hard policy choice to immunize everyone • Cons • Requires lots of staff • Requires quarantine • Requires lots of time • Chance of breakout
Contact Tracing Model and Lessons from Katrina • National Security Administration Course Problem • How much do the feds depends on the states to do their part? • What is the risk if the states do not do their part? • How can the feds know in time? • No one was interested • Of course the states will do what they are required to do • What else can the states say when they depend on federal money?
Political Choices are Hidden in the Models • Federal policy is based on a low transmission rate • Is that justified by the data? • Is the potential upside risk too great with this assumption? • Dark Winter is based on a high rate • Do anything and pay anything to avoid bioterrorism • Convenient for bioterrorism industries
The Problem • Smallpox is still a real threat • Or is it? • The CDC plans for dealing with an outbreak are completely unrealistic • Should we start vaccinating the population? • Vaccinating health care workers alone is not epidemiologically sound or politically acceptable • How do we resolve the uncertainty?