Download
1 / 36
460 likes | 723 Views
Corneal Disease. Anatomy of the Eye. Thygeson’s Superficial Punctate Keratopathy. Symptoms Foreign-body sensation Photophobia Tearing No history of recent conjunctivitis Usually bilateral and has a chronic course with exacerbations and remissions.

E N D
Thygeson’s Superficial Punctate Keratopathy • Symptoms • Foreign-body sensation • Photophobia • Tearing • No history of recent conjunctivitis • Usually bilateral and has a chronic course with exacerbations and remissions
Thygeson’s Superficial Punctate Keratopathy • Critical sign: • Course punctate gray-white corneal epithelial opacities, often central with minimal or no staining with fluorescein
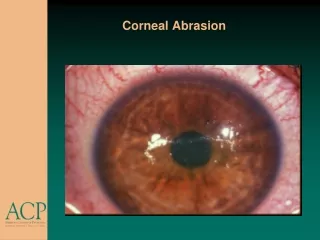
Corneal Abrasion • Symptoms: • Pain • Photophobia • Foreign-body sensation • Tearing • History of scratching the eye
Corneal Abrasion • Critical sign: • Epithelial staining defect with fluorescein • Other signs: • Conjunctival injection • Swollen eyelid • Mild anterior-chamber reaction
Work-up: Slit-lamp exam Use fluorescein Measure size of abrasion Diagram its location Evaluate for anterior-chamber reaction Evert eyelids and make certain no further FB Treatment: Non-contact lens wearer: Cycloplegic Antibiotic ointment or drops Contact lens wearer: Cycloplegic Tobramycin drops 4-6x/day Corneal Abrasion
Follow-up Non-contact lens wearer with a small-noncentral abrasion: Ointment/drops x 5 days Return if symptoms worsen Central or large abrasion: Recheck 24 hours If improvement, continue top abx If no change, repeat initial treatment Follow-up: Contact lens wearer Recheck daily until epithelial defect resolves May resume contact lens wearing 3-4 days after eye feels completely normal. Corneal Abrasion
Corneal Foreign Body • Symptoms: • Foreign-body sensation • Tearing • Blurred vision • Photophobia • Commonly, a history of a foreign body
Corneal Foreign Body • Critical sign: • Corneal foreign body, rust ring, or both. • Other signs: • Conjunctival injection • Eyelid edema • Superficial Punctate Keratitis (SPK) • Possible small infiltrate
Work-up: History – metal, organic, finger, etc Visual acuity before any procedure Slit-lamp With history of high velocity FB – dilate the eye and examine the vitreous and retina Treatment: Topical anesthetic Remove foreign body Remove rust ring (Ophthalmology recommended) Document size of epithelial defect Cycloplegic Antibiotic ointment/drops Corneal Foreign Body
Corneal Foreign Body • Follow-up: • Small (<1-2 mm in diameter), clean, noncentral defect after removal: antibiotics for 5 days and follow-up as needed. • Central or large defect or rust ring: follow-up ophthalmology within 24 hours to reevaluate.
Corneal Laceration • Partial-thickness laceration • The anterior chamber is not entered and, therefore, the globe is not penetrated
Corneal Laceration • Work-up: • Complete ocular examination • Slit-lamp to rule out ocular penetration • IOP • Seidel test • Fluorescein stain over site shows streaming. + full thickness.
Treatment: Intact anterior chamber Cycloplegic Antibiotic Ophthalmology follow-up Ruptured anterior chamber Immediate optho consult Follow-up: Reevaluate daily until healed Corneal Laceration
Other signs: No conjunctival injection No corneal edema Treatment: Mild: Artificial tears Moderate/severe Mild topical steroid for 1 week, then taper slowly. Follow-up Every week during exacerbations, then every 3-12 months If on topical steroids, check IOP Thygeson’s Superficial Punctate Keratopathy
Pterygium • Patients present with complaint of tissue growing over their eye. • Caused by exposure to ultraviolet light • More commonly encountered in warm, dry climates or smoky/dusty environments.
Pterygium • Symptoms: • Irritation • Redness • Decreased vision • Usually asymptomatic
Critical signs: Wing-shaped fold of fibrovascular tissue arising from the interpalpebral (90%) conjunctiva and extending onto the cornea Work-up: Slit-lamp exam to identify lesion. Treatment Protect eyes from sun, dust, and wind Artificial tears, mild vasoconstrictor or topical decongestant/ antihistamine combination Moderate/severe – mild topical steroid Pterygium
Pterygium • Follow-up • Asymptomatic patients may be checked every 1-2 years • If treating with topical vasoconstrictor, the check in 2 weeks. Discontinue when inflammation subsides. • If topical steroid, check 1-2 weeks and check IOP. Taper and discontinue over several days once resolution.
Infectious Corneal Infiltrate/Ulcer • White infiltrate/ulcer that may/may not stain with fluorescein must always be ruled out in contact lens patients with eye pain. • Can occur in patients with recent history of eye trauma. • Slit-lamp beam cannot pass through infiltrate.
Infectious Corneal Infiltrate/Ulcer • Symptoms: • Red eye • Mild-to-severe ocular pain • Photophobia • Decreased vision • Discharge
Critical sign: Focal white opacity in the corneal stroma Other signs: Conjunctival injection Inflammation surrounding infiltrate Corneal thinning Possible anterior-chamber reaction Etiology: Bacterial Fungal Acanthamoeba (contact lens wearers) Herpes Simplex Virus Infectious Corneal Infiltrate/Ulcer
Work-up: History: contact lens wear and regimen, trauma, foreign body. Slit-lamp exam: stain with fluorescein to assess epithelial loss. Document size, depth, and location. Assess anterior chamber Check IOP Treatment: Generally treated as bacterial unless there is a high index of suspicion for another form. Cycloplegic Topical antibiotics No contact wearing Pain med if needed Ophthalmology consult Infectious Corneal Infiltrate/Ulcer
Herpes Simplex Virus • Symptoms: • Usually unilateral red eye • Pain • Photophobia • Tearing • Decreased vision • Skin rash
Herpes Simplex Virus • Work-up: • History: • Previous episode • Contact lens • Recent steroids • External exam • Slit-lamp with IOP • Dendritic lesion • Check corneal sensation prior to anesthetic • Viral culture
Herpes Simplex Virus • Treatment: • Topical acyclovir tid • Warm soaks tid (if eyelid involved) • Ophthalmology referral • (oral acyclovir if primary herpetic disease)
Slit Lamp Examination • Extremely useful instrument • Can reveal pathologic conditions that would otherwise be invisible • Permits detailed evaluation of external eye injury and is definitive tool for diagnosing anterior chamber hemorrhage and inflammation
Slit Lamp Examination • Indications: • Diagnosis of abrasions, foreign body, and iritis • Facilitate foreign body removal • Contraindicated: • Patients who cannot maintain upright position, unless using portable device
Slit Lamp Examination • Set up • Patient’s chin is in chin rest and forehead is against headrest • Turn on light source • Low to medium light source is appropriate for routine exam • Start on low power microscopy
Slit Lamp Examination • 1ST setup: • For examination of right eye, swing light source out 45º. • Slit beam is set at maximum height and minimal width using white light. • Scan across at level of conjunctiva and cornea, then push slightly forward and scan at level of iris.
Slit Lamp Examination • Basic setup used to examine for: • Conjunctiva traumatic lesions • Inflammation • Corneal FB • Lids for • Hordeolum • Blepharitis • Complete lid eversion • Examine undersurface
Slit Lamp Examination • 2nd setup: • Same as first, only uses blue filter. • Beam is widened to 3 or 4 mm. • Examine for uptake of fluorescein.
Slit Lamp Examination • 3rd setup: • Search for cells in anterior chamber. • Height of beam should be shortened to 3 or 4 mm. • Switch to high power. • Focus on center of cornea and the push slightly forward, focus on anterior surface of lens • Keep beam centered over pupil. • Look for searchlight affect in anterior chamber