Download
1 / 35
490 likes | 1.98k Views
Embolism, Infarction and Shock. Dr Raihan Sajid msajid@alfaisal.edu. Embolism. Embolism A mass of material [ embolus ] that can move in the vascular system and become lodged in some vessel and block its lumen Most emboli are derived from thrombus

E N D
Embolism, Infarction and Shock Dr Raihan Sajid msajid@alfaisal.edu
Embolism • Embolism • A mass of material [embolus] that can move in the vascular system and become lodged in some vessel and block its lumen • Most emboli are derived from thrombus • Most commonly pulmonary embolism from venous thrombosis in deep leg veins(DVT)
Types of embolus • Thromboembolism (the most common! >90%) • Others • Atheromatous emboli • Amniotic fluid (parturition) • Air/Gas (crime novels and deep sea divers) • Fat (trauma, especially fractured long bones) • Tumour (metastasis) • Foreign material (i.v. drug abusers) • Infective agents (infected heart valves)
Pulmonary embolism • 95% of venous thrombosis is in the deep leg veins • the rest in deep pelvic veins or • intra cranial venous sinuses • Most emboli from such sources will therefore travel in the blood stream and arrest in the first vascular bed they meet . . . in the lungs . . . hence pulmonary embolism
Large embolus derived from a lower extremity deep venous thrombosis and now impacted in a pulmonary artery branch.
Effects of pulmonary embolism Mainly dependant on size • Small emboli may go unnoticed and lyse • May organise and cause some minor reduction in lung function • If numerous, small emboli can cause quite marked reduction in lung function over time • Medium sized emboli can cause significant acute respiratory and cardiac problems including shortness of breath, haemoptysis, heart failure • Large emboli can cause sudden death (saddle embolus)
Prevention of pulmonary embolism • Prevention of pulmonary embolism depends on preventing venous thrombosis in the legs • Risk factors (Virchow’s triad) • Immobilisation - Bed rest • Surgery - Hyper-coagulable blood • Obesity - Pregnancy • Reduce and remove risk factors • Including elastic stockings, early mobilisation • and anticoagulation
Systemic (arterial) embolism • Arise in the arterial system • Effects depend on • size of the emboli, • their number • the size of the vessels • the nature of the tissue • Most commonly arise from the heart or great vessels (eg. atheroma in aorta)
Common sites of infarction as a consequence of arterial emboli
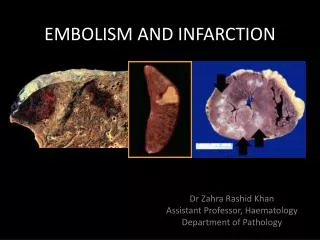
Infarction Dr Raihan Sajid msajid@alfaisal.edu
Definition • An infarct is an area of ischemic necrosis caused by occlusion of either the arterial supply or the venous drainage in a particular tissue • •Nearly 99% of all infarcts result from thromboembolic events ,and almost all result from arterial occlusion.
Infarcts are classified on the basis of their color (reflecting the amount of hemorrhage) and the presence or absence of microbial infection • Red (hemorrhagic) infarcts occur • with venous occlusions (such as in ovarian torsion) • In loose tissues (such as lung) • In tissues with dual circulations (e.g. lung and small intestine).
White (anemic) infarcts occur • With arterial occlusions in solid organs with end-arterial circulation (such as heart ,spleen ,and kidney) • Solid tissues
Examples of infarcts. Hemorrhagic, roughly wedge-shaped pulmonary infarct. Sharply demarcated white infarct in the spleen.
The dominant histologic characteristic of infarction is ischemic coagulative necrosis • Most infarcts are ultimately replaced by scar tissue. • The brain is an exception to these generalizations ; ischemic injury in the central nervous system results in liquefactive necrosis
Remote kidney infarct, now replaced by a large fibrotic cortical scar.
Septic infarctions • Septic infarctions may develop when embolization occurs by fragmentation of a bacterial vegetation from a heart valve or when microbes seed an area of necrotic tissue.
Definition • Shock, or cardiovascular collapse, is the final common pathway for a number of potentially lethal clinical events, including severe hemorrhage , extensive trauma or burns, large myocardial infarction, massive pulmonary embolism, and microbial sepsis.
Gives rise to systemic hypo-perfusion caused by reduction in: • Cardiac output • The effective circulating blood volume. • The end results are hypotension , followed by impaired tissue perfusion and cellular hypoxia.
Less commonly: • Neurogenic shock-in the setting of anesthetic accident or spinal cord injury, owing to loss of vascular tone and peripheral pooling of blood. • Anaphylacticshock, initiated by a generalized IgE- mediated hypersensitivity response, is associated with systemic vasodilatation and increased vascular permeability
Clinical course • The clinical manifestations depend on the precipitating insult. • In hypovolemic and cardiogenic shock, the patient presents with hypotension; a weak, rapid pulse; tachypnea; and cool, clammy, cyanotic skin. • In septic shock, the skin may initially be warm and flushed because of peripheral vasodilation
Stages of shock • Non-progressive (compensated) • Compensatory mechanisms? • (baroreceptor reflexes, release of catecholamines, activation of renin angiotensin axis, ADH release, generalized sympathetic stimulation) • Progressive (organ hypoperfusion) • Irreversible (end organ failure)
Morphological changes • Changes of hypoxic injury and micro-thrombi in any tissue particularly in brain, heart, lungs, kidneys, gastrointestinal tract. • Kidneys: ATN • Lungs: Diffuse alveolar damage • Skin: Petechial hemorrhages
Clinical manifestations of shock • Warm shock • Fever • flushed skin • Tachycardia • Hypotension (systolic < 100 mmHg),wide pulse pressure (bounding pulse) Cold shock • Cold and clammy skin • Tachycardia • Hypotension (systolic < 100 mmHg), narrow pulse pressure
Clinical manifestations of shock • Cyanosis and hypoxemia • Altered sensorium, irritability • Oliguria • Acidosis • Mottling • Signs of multisystem organ failure
Diagnosis • Symptoms • A significant drop in blood pressure • Low urine output and • Blood tests that reveal acidic blood with a low carbon dioxide