Download
1 / 29
290 likes | 416 Views
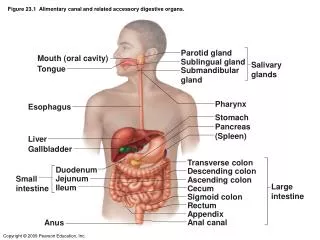
Case Presentation : Tracheal obstruction by calcified TB gland in a child. Aneesa Vanker, Pierre Goussard, Sharon Kling, JT Janson, B Barnard, M Connellan . Tygerberg Children`s Hospital.Department of Paediatrics and Cardiothoracic surgery .University of Stellenbosch. Background.

E N D
Case Presentation : Tracheal obstruction by calcified TB gland in a child Aneesa Vanker, Pierre Goussard, Sharon Kling, JT Janson, B Barnard, M Connellan . Tygerberg Children`s Hospital.Department of Paediatrics and Cardiothoracic surgery .University of Stellenbosch
Background • 9 month old baby GA referred from Worcester Hospital • Problems: # Recurrent “stridor” for 3 months # Pulmonary tuberculosis on treatment for 5 months
TB diagnosis & Mx • TB diagnosed at 4 months of age based on - +ve tuberculin skin test - CXR with suggestive features of TB - No gastric washings done • Commenced on TB Rx and was already on continuation phase Rx • Apparently “many” TB contacts
Stridor background • History of repeated admission to Caledon Hospital from 6 months of age with stridor. • Treated with nebulisations and sent home. • Eventually at 9 months of age, referred to Worcester Hospital for Ix of stridor. • Noted on CXR to have ?mass in right main bronchus area
TCH course • Clinically: Well grown child on 10th centile for weight. Resp exam: Monophonic wheeze Minimal stridor No differential air entry Other systems normal
Investigations • CXR – calcified lesion in area of right main bronchus – most likely lymph node • ENT consult – Not able to detect any abnormality • The next step - Bronchoscopy
Bronchoscopy • Large gland herniating into the trachea with >90% occlusion • Right main bronchus occluded by herniating gland • Areas of gland removed piecemeal at bronchoscopy (endoscopic enucleation)– still significant occlusion • BAL done and cultures sent
Further developments • Intubated post bronchoscopy to protect the airway • Transferred to PICU • Urgent chest CT scan done confirmed large gland of tuberculous nature herniating into trachea and right main bronchus
Surgery • Enucleation done • Large amount of caseous material removed • Small tracheal defect closed
Post-surgery • Repeated bronchoscopy 1 hour after returning to PICU • Trachea now only 50% occluded (prev >90%), RMB still occluded • Changed to MDR TB Rx (INH, Rif, Oflox, Amik, Etham) + Steroids • Reason – no response to previous Rx, possible MDR TB • Extubated
Post surgery Before surgery
Further course • ZN stain positive for AFB on enucleated gland • Culture pending • Clinically wheeze improved • Repeat bronchoscopy 1 week post-enucleation Trachea patent, no gland herniation, RMB only 50% occluded by herniating gland
Transferred back to Worcester to continue TB treatment • For follow-up in 1 months time
Airway involvement in TB • Trachea and 2 main bronchi most affected. • Upper airway involvement rare in children
Presentation • Enlarged glands can cause external compression of the airways. • May herniate into airways. • Varying degrees of obstruction rarely complete obstruction. • Partial obstruction “ball-valve” effect – air enters lung but trapped on expiration • Complete obstruction lung or lobar collapse
Assessment • CXR – 4 patterns of compression 1) airway narrowing 2) ball-valve effect 3) expansile pneumonia 4) lobar collapse • Bronchoscopy – degree of obstruction, BAL, endoscopic enucleation • CT scan – Confirmation, assist in planning further interventions
Management • TB treatment – standard 3 drug regime • Corticosteroid – prednisone 2mg/kg for 1 month then weaned • Evaluated for enucleation – life-threatening obstruction, poor response to Rx and steroids.
Learning points • Differentiating stridor from monophonic wheeze • Stridor - Harsh, high-pitched inspiratory sound usually audible without a stethoscope - Extrathoracic obstruction • Monophonic wheeze – Intrathoracic obstruction
Recurrent presentations of stridor/wheezing warrant further investigation • Although on CXR – gland look calcified, still needed further management • TB cultures are always important especially when the diagnosis is made
Summary • Unusual presentation of endobronchial TB. • Potential for life-threatening complications. • Thus far the outcome has been favourable.
Review of the literature • Endobronchial TB with gland herniation has been described: Airway involvement in pulmonary tuberculosis. Goussard P, Gie R Paediatr Respir Rev. 2007 Jun;8(2):118-23. • However, very little described on gland herniation into the trachea • 2 articles : Tuberculous cavitating node communicating with the trachea. Case report with radiographic and pathologic review. Palacios EJ, Tirman RM, White HJ. J Ark Med Soc. 1972 May;68(12):407-9. Airway obstruction secondary to tuberculosis lymph node erosion into the trachea: drainage via bronchoscopy. Schwartz MS, Kahlstrom EJ, Hawkins DB. Otolaryngol Head Neck Surg. 1988 Dec;99(6):604-6.