Download
1 / 34
350 likes | 466 Views
CCMs and PRs structure and functions & civil society opportunities. The Global Fund philosophy.

E N D
CCMs and PRs structure and functions & civil society opportunities
The Global Fund philosophy « The Global Fund recognizes that only through acountry-driven, coordinated and multi-sectoral approach involving all relevant partners will additional resources have a significant impact on the reduction of infections, illness and death from the three diseases. Thus, a variety of actors, each with unique skills, background and experience, must be involved in the development of proposals and decisions on the allocation and utilization of Global Fund financial resources. To achieve this, the Global Fund expects grant proposals to be coordinated among a broad range of stakeholdersthrough a Country Coordinated Mechanism (CCM) and that the CCM will oversee the implementation of approved proposals. » CCM Guidelines, GF, p. 1
What is a CCM? « CCMs are partnerships comprised of representatives from both the public and civil society sectors who coordinate the submission of one national proposal based on priority needs. Additionally, CCMs are responsible to oversee the progress of program implementation…The CCM [is] a central pillar of the Global Fund’s architecture to ensure country-driven, coordinated, and multi-sectoral processes for leveraging and effecting additional resources …to fight AIDS, TB and malaria.» Clarifications, GF, p. 1
Key Principles of CCMs Multi-sectoral partnership Broad participation Non-government representatives Consensual decision- making Transparency Documentation Active communication and consultation with stakeholders Grant oversight
CCMs: Six Minimum Criteria • Transparent selection process for CCM nongovernmental members • Membership of persons affected by HIV/AIDS, TB, and malaria • Transparent and documented process to solicit and review proposal submissions • Transparent and documented process for nominating the PR and overseeing program implementation • Ensure the input of a broad range of stakeholders • Have a written conflict-of-interest plan, especially when the CCM chair or vice chair represents the same institution as the principal recipient
CCM Composition At least 40% of CCM seats Government Education/Universities NGOs, CBOs Assoc. of people living w. diseases Private sector FBOs, religious leaders Bilateral and multilateral development partners Key affected populations Attention required to gender balance on the CCM ! Attention required to geographical representation on the CCM !
CCMs: Principal Responsibilities Identify national priorities and gaps in programmatic, technical, & geographic coverage or financial support Promote multi-sectoral participation Ensure the harmonization of Global Fund grants with other support for the three diseases Coordinate and ratify grant proposals Designate the Principal Recipients Ensure grant oversight and evaluate Phase 2 progress Resolve problems surpassing the authority & competence of Principal Recipients Submit Phase 2 and Rolling Continuation Channel requests Ensure transparency with stakeholders and the Global Fund
CCM: A national, representative, multi-sectoral governance body Members represent their constituency, not themselves or their institution. The CCM governs in the national interest. The CCM neither manages nor executes Global Fund grants.
The 5 Key Functions of a CCM 2. Harmoni-zation of GF funds with other resources 1. Organization & functioning of the CCM & its Secretariat 4. Oversight of grants & Principal Recipients 5. Documen-tation & communi-cation with constituen-cies & GF 3. Proposal develop- ment
CCM Oversight Every CCM should be able to answer these questions about each grant: Where is the money ? Where are the drugs, commodities, equipment? Are SRs receiving the resources they require? Are the projects being carried out as planned? What are the results; is the grant on target?
CCMs: Frequent Problems Under-designed as structures Conflicts of interest Dominated by the Minister of Health or public & health sectors Poor representation of sectors (members believe they represent only their organization; motivation is to ensure my organization gets GF funds) Confusion between the CCM and other national bodies Lack of political will Poor or non-existent oversight, little support of PRs to resolve cross-cutting problems & bottlenecks
Who can be a PR? Government ministry or agency, or National AIDS Commission National NGO, faith-based organization, or foundation Multilateral agency (e.g., UNDP, UNICEF) International PVO with in-country presence (e.g., Red Crescent, CARE, PACT, PSI) Private-sector organization
CCM & PR: Boundaries • PR selects SRs if they were not chosen during proposal development • The GF negotiates directly with the future PR before signature, once the PR passes the PR assessment • PR manages the grant • PR submits quarterly reports directly to the LFA • PR resolves grant problems or asks the CCM for help • PR ensures transparency and communicates grant results • PR and SRs develop reprogramming, Phase 2 and RCC requests CCM designates the PR, manages & validates the proposal CCM is responsible for the proposal until the GF approves the new PR CCM oversees implementation CCM resolves systemic problems and bottlenecks the PR cannot solve CCM ensures transparency of its activities, decisions, and proposal development CCM approves requests to reprogram funds, for Phase 2, RCC
Sub-Recipients &Sub-Sub-Recipients SSR SSR SSR
CSOs Can Serve . . . • On the Country Coordinating Mechanism (CCM) • As Principal Recipients (PR) • As Sub-Recipients (SR) • As Sub-Sub-Recipients (SSR) • As contractors or service providers
Who can be an SR? Government ministry or agency, or AIDS commission National NGO, FBO, Foundation Multilateral agency (UNDP, UNICEF) International PVO with in-country presence (e.g., Red Crescent, CARE, PACT, PSI) Private-sector organization (Shell Philippines) As long as they are selected by the CCM or the PR and can pass the Global Fund assessment.
SRs May Have One or More SSRs How the Global Fund envisioned the SRs: Locally present stakeholder institutions from all sectors Project implementers
Types & Numbers of SRs in 10 Countries (by Disease) Source: Global Fund TERG 5-year Evaluation, Nov. 2008
Selection and Roles of Sub-recipients Selection during proposal development: strategic advantage, named in the proposal Technical expertise, special expertise or authority Geographic coverage or niche targeting More accurate targets and budgets Roles for sub-recipients Lead sub-recipients Coordinating sub-recipient Sub sub recipients Participation in strategic design, setting targets, defining roles for each partner institution Participation In final pre-signature planning & negotiations Participation In monitoring and evaluation of performance Sub-sub-recipients Participation In technical execution of activities
Some Expectations and Requirements of SRs and PRs • Sr’s • Annual work plans • Half-year/quarterly financial and progress update reports on time • Adherence to GF and national requirements • Adherence to the work plan • Transparency PR Agreements/MoUs clarifying roles and responsibilities Timely disbursements Operations manual to guide grant implementation Technical support Grouped procurement Transparency
How Civil Society can be effectively involved in Global Fund processes
Who do we mean by civil society? ● International Non-Governmental Organisations ● Associations of people living with the diseases ● Associations of people using drugs ● National and local NGOs ● Community Based Organisations ● Faith Based Organisations ● Trade Unions ● Womens‘ organisations ● Youth Organisations ● Organisations supporting people with disabilities
The principle of „GIPA“ = To „support a greater involvement of people living with HIV/AIDS at all...levels...and to...stimulate the creation of supportive political, legal and social environments.“ ● Endorsed by United Nations Member countries. ● Binding the expertise of PLWHAs. ● Support acceptance and preparedness. ● Enhance the effectiveness of services.
Why would we work with Civil Society? ● Reach beyond the formal infrastructure ● Provide services to hard-to-reach communities ● Involve people living with the diseases ● Contribute to a wholistic approach ● React relativelyflexible to new challenges and changes ►Evidence of civil society as strong implementers of programs at the country level. ►Programs with strong civil society involvement achieve very good results. ►► Collaboration with civil society adds value.
The Added Value of Civil society • Innovation in health service delivery for key affected populations • Rapid response in terms of prevention, treatment and advocacy programs • Importance of CS in roll-out/scale-up of treatment literacy • Scaling-up prevention among key affected populations • National HIV Plans: represent the best speaker on community needs
Civil society in MENA Advocacy, raising awareness and fighting stigma and discrimination. Pioneer in establishment of programs for key affected populations: IDU (Algeria, Egypt, Iran, Lebanon, Libya, Morocco, Syria) Migrants and refugees (Algeria, Djibouti, Morocco, Somalia, Sudan, Yemen) Sex work (Algeria, Egypt, Iran, Lebanon, Morocco, Somalia, Syria, Tunisia) MSM (Morocco, Pakistan, Algeria, Lebanon, Tunisia,) Pioneer in delivering VCT services (Morocco and Algeria) and treatment literacy programs (Morocco)
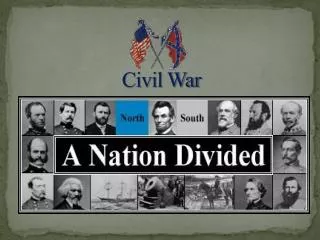
Health Services Pyramid 80% of resources 20% of population Tertiary Health Care Secondary Health Care Majority of population DTF Primary Health Care CSS Community Based Health Services
Civil Society in the Global Fund The Fund will support programs that Global Fund Framework Document, 2002
Governance CCM members Board members Implementers Grant Oversight Watchdogs Non-Government Organizations Affected and Most-at-Risk Populations Faith-Based Organizations Advocates Community-Based Organizations Program Design Dual Track Financing PRs, SRs, SSRs Early Warning
Entry points for civil society engagement in grant implementation • Engagement in/through CCM • Proposal development • New Round of funding • Phase 2 • RCC • Ongoing oversight • Identifying challenges • Developing responses involving CSOs Through NGO representation on CCM • Implementation • PR (dual-track financing) • SR Grant Signing Proposal Development Phase 2 RCC 0 1 2 3 4 5 • Phase 2 Request • Addressing challenges through CCM • Including CSOs as SRs for implementation • Proposal Development • Defining key affected populations where necessary • Identifying gaps in current activities • Developing strategies and interventions • Including focus on CSS activities • Including CSOs as SRs • RCC Proposal Development • Defining key affected populations where necessary • Identifying gaps in current activities • Developing strategies and interventions • Including focus on CSS activities • Including CSOs as SRs