Download
1 / 47
470 likes | 550 Views
Explore the complexities influencing HIV prevalence in Black men who have sex with men and the impact of social, behavioral, and demographic factors on infection rates. Gain insight into disparities in diagnosis and risk factors within this community.

E N D
High rates of HIV infection in the absence of greater risk among Black MSM Greg Millett Centers for Disease Control Division of HIV/AIDS Prevention The findings and conclusions in this report are those of the authors and do not necessarily represent the views of the Centers for Disease Control and Prevention
Race/ethnicity of MSM Diagnosed with HIV, 2005 1% 19% 32% 46% Source: Centers for Disease Control and Prevention. “HIV/AIDS among Men who have Sex with Men.” Fact Sheet. June 2007.
HIV Diagnoses by Age HIV Dx among MSM ages 13-24 • (MMWR, 2001; MWWR, 2005)
HIV Diagnosis & AIDS Mortality Diagnosed later in infection (Wortley et al., 1995) Quicker disease progression (Blair et al., 2002; Hall et al., 2007) Mortality (era after HAART) • 1996-1998 (Blair et al., 1995) • 1996-2002 (Hall et al., 2007)
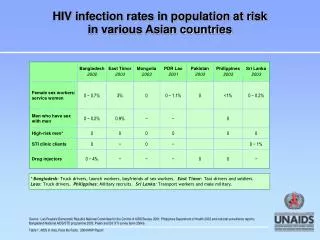
Gonorrhea, Chlamydia, Syphilis and HIV among men who have sex with men, byrace/ethnicity, STD clinics, 2005 • *Excludes persons previously known to be HIV-positive. • Seroreactivity.
HIV/STD Coinfection • Among 4000 MSM tested between 1990 and 1999 in NYC (Torian et al., 2002) • HIV+ Black MSM more likely than HIV+ White MSM to be coinfected with Gc, syphilis or nongonococcal urethritis (60% vs. 18%)
HIV M-to-F Transgender Meta-anlysis • Analysis of 29 studies and 2700 transgender individuals (Herbst et al., 2007) • Overall HIV seropositivity 28%
HIV M-to-F Transgender Meta-anlysis • Analysis of 29 studies and 2700 transgender individuals (Herbst et al., 2007) • Overall HIV seropositivity 28% • By race/ethnicity • Latinos 16% • White 17% • Black 56%
Does individual risk behavior drive the epidemic among Black MSM?
Unprotected anal intercourse • Substance use (during sex and/or injection) • Crack/ Cocaine • Heroin • Poppers • Meth
Research Paradox “established risk factors for HIV infection in homosexual/ bisexual men do not explain the differences in HIV seroprevalence or seroconversion rates between blacks and whites.” Samuel et al., 1987
NHBS Amphetamine Use (past 12 mos) Data collection 2003 -2005 (17 MSAs) (n = 4510) (n = 2680) (n = 1739) (n = 449)
ByH Meth Use (Past 3 mos) Data collection 2005 -2006 (3 cities) n=1014 n=1148
Young MSM (ages 15-22): Substance Use Behavior (Harawa et al., 2004) *P< .05
Substance Use Across 20 Studies Compared with Black MSM, White MSM across studies: • 3 times more likely to use amyl nitrites • 54% more likely to use drugs associated with HIV infection (IDU, amphetamines, crack/cocaine, needle sharing, opiates, nitrites) • 40% more likely to use any illegal substance (Millett et al., 2007)
Young MSM (ages 15-22): Sexual Risk Behavior Yet compared with White MSM in this sample: Black MSM were 9 times more likely to be HIV-positive (Harawa et al., 2004) *P< .05
NHBS: Sexual Risk (ages18-81) n= 4510 n= 2680 n= 1739 (CDC, 2006)
NHBS: HIV Prevalence by Race (MMWR, 2005)
Unprotected Anal Intercourse Across 17 Studies • Comparable rates of UAI by time period • Comparable rates of receptive UAI • Comparable rates of UAI with ‘known’ HIV-positive partners • Comparable rates of sex trade (Millett, 2007)
What does (and does not) place Black MSM at risk for HIV infection?
Social/ Structural Interpersonal/ Network Individual
Black MSM 70% less likely to identify as gay(Millett, 2007) 60% less likely to disclose sexuality(Millett, 2007) Less likely to join gay org or read gay media(McKirnan, 1995; Stokes, 1996; Kennamer, 2000) Sexual risk with male partners and HIV prevalence is higher among gay ID men compared with nongay-ID (Wood, 1993; Pathela, 2006) Sexual risk with male partners and HIV prevalence is greater among disclosing rather than nondisclosing MSM (CDC, 2003) HIV infection by sexual identity 1100 Black MSM Bisexual men 76% less likely Heterosexual men 91% less likely(Millett, 2007) Individual-LevelDemographic Factors: Gay ID/ Disclosure
Individual-LevelDemographic Factors: Undiagnosed HIV • Greater rates among Black and Latino MSM • Ages 15-22: Black 91%, Latino 69%, White 60% (MacKellar et al., 2005) • Ages 18-81: Black 67%, Latino 48%, White 23% (CDC, 2005) • Known positives engage in fewer sexual risk behaviors with negative or unknown status partners (Colfax et al., 2002) • People with unrecognized infection primarily responsible for ongoing epidemic (Marks et al, 2006)
Individual-Level Psychological Factors: Abuse, Distress • History of sexual abuse associated with sexual risk (Fields, 2007; Wheeler, 2007) • Depressive distress associated with greater rates of sexual risk (Crawford, 2002; Myers, 2003)
CCR5 base 32 allele Protective against HIV infection (Marmor, 2001; Stephenson, 2001) Slower disease progression (Huang, 1996; Michael, 1997) <.1% of non-Whites (Martinson, 2000) Few studies of MSM and none of MSM of color (Millett, 2006) STI Increases risk of HIV infection or transmission (Flemming, 1999): Meta-analysis(Millett, 2007): Black MSM 2x more likely to be dx with a current STD 50% more likely to have GC 2x more likely to have syphilis Individual-LevelBiological Factors: Immunogenetics and STI
Individual-LevelBiological Factors: Circumcision • General population • Prevalence: White (81-88%), Black (65-73%), Latinos (42-54%)(Xu, 2007; Laumann, 1997) • MSM • Protects insertive partner only • 1 US examined circumcision among Black MSM. No association among (Millett, 2007) • Black MSM • Black MSM-only • Black MSM/W • Black MSM who reported only being tops
Negative peer norms toward condom use associated with greater rates of UAI (Bakeman, 2007; Jones, 2007; Hart & Peterson, 2004; Peterson, 1995) Gay ID associated with negative peer norms toward condom use and safer sex communication (Jones, 2007) Interpersonal Level: Communication/ Peer norms
Negative peer norms toward condom use associated with greater rates of UAI (Bakeman, 2007; Jones, 2007; Hart & Peterson, 2004) Gay ID associated with negative peer norms toward condom use and safer sex communication (Jones, 2007) Interpersonal Level: Communication/ Peer norms Sex with older male partners(Bingham, 2003) Intraracial sexual mixing(Bingham, 2003; CDC, 2003)
Interpersonal Level: Social Support/ Partner status • Social support: • Lower levels of social support associated with greater risk taking (Peterson, 1992) • Inverse relationship between social support and sexual risk among HIV-positive Black MSM (Ostrow, 1991) • Main vs. casual partner • Men with a main partner more likely to engage in insertive or receptive sex (Hart & Peterson, 2004)
Social/Structural Level:Poverty/ Healthcare • Poverty • Black MSM: Lower income associated with greater likelihood of HIV infection (Peterson, 1992; Mays, 1995) • Healthcare access/ utilization • Access: No differences in health insurance (Halkitis, 2003; Kass, 1999) • Utilization: HIV-positive Black MSM 57% less likely to access ART compared with HIV-positive White MSM (Millett, 2007) • Adherence: Less likely to adhere to meds (Kleeberger, 2001 & 2004)
Social/ Structural: Gay-related Development and Early Abuse ,,,, (Friedman, 2007)
Social/ Structural: Gay-related Development and Early Abuse ,,,, (Friedman, 2007) • Men who reported earlygay-related development were more likely to report • Harassment for being gay during childhood and adolescence • Sexual abuse (> once) during childhood and adolescence
Social/ Structural: Gay-related Development and Adult Health Outcomes (Friedman, 2007)
Social/Structural Level:Discrimination • History of discrimination associated with greater sexual risk (Zamboni, 2006) • Relationship also mediated by psychiatric symptoms
Traditional risk factors for HIV infection (UAI, substance use) are not similar for Black MSM and other MSM • Must address structural and interpersonal factors since individual risk does not explain HIV disparities among Black MSM
Create new behavioral interventions specific to Black MSM • Must partner with communities • Tailor existing effective behavioral interventions for MSM for Black MSM populations • Black MSM are not homogenous (i.e. drug use by coast, multiethnic vs not) • Investigate applicable biological interventions (PrEP, rectal microbicides, etc)
Encourage frequent HIV/STI screening (every 6 mos) • Link HIV-positive MSM (especially Black MSM) with appropriate care • Target gay-identified, ‘out’ men, MSM
Support men throughout their lifetime, not just when they are young • Focus on the whole person • Operate from an ‘asset’ rather a ‘deficit’ model (resiliency)
Amphetamine use (past 5 years) Black MSM: East vs. West Coast (n = 472) (n = 2202) (Sullivan, 1998)
YMS: Meth Use (Lifetime) Black MSM vs. Mixed MSM (n = 814) (n = 201) (Harawa, 2004)
YMS: Black vs. Multi-ethnic (Harawa, 2004)