Download
1 / 20
200 likes | 212 Views
PREVALENCE OF HIV/HBV/HCV CO-INFECTION AMONG PWID, FSW, MSM IN VIETNAM. Ass. Prof. Nguyen Anh Tuan, MPH, PhD National Reference Laboratory - HIV/AIDS Department National Institute of Hygiene and Epidemiology. Global Context.

E N D
PREVALENCE OF HIV/HBV/HCV CO-INFECTION AMONG PWID, FSW, MSM IN VIETNAM Ass. Prof. Nguyen Anh Tuan, MPH, PhD National Reference Laboratory - HIV/AIDS Department National Institute of Hygiene and Epidemiology
Global Context • Viral hepatitis is a leading communicable cause of death (GBD, Lancet 2015) • World Health Assembly Hepatitis Resolutions passed in 2010 and 2014 • Hepatitis listed alongside HIV, TB, and malaria in post-2015 sustainable development goals “End the epidemics of AIDS, TB, malaria and .. combat hepatitis, water-borne diseases and other communicable diseases” • New medicines sparking treatment ‘revolution’
Vietnam Epidemic Estimated 6 million with chronic HBV infection by 2020 Viral hepatitis 3rd leading cause of death in Vietnam; HBV and HCV major causes (GBD, Lancet 2015) High prevalence of HBV: 6 – 25% in general population (Van TTN, APJPH 2012). HCV concentrated among PWID (Nadol et al. Plos One 2015)
Viral Hepatitis Strategic Information • Viral hepatitis strategic information has many purposes and methods • Viet Nam currently uses case reporting to detect outbreaks • Viet Nam also exploring sustainable approaches for estimating disease burden nationally, regionally, and in different populations using surveys Wiktor. 2015
Hepatitis Case Reporting System Policy • Viral hepatitis is one of the 28 notifiable diseases in Viet Nam • Circular 13/2013/TT-BYT provides guidance on infectious disease surveillance, including viral hepatitis • System provides estimates of cases detected and reported in health facilities Challenges • Specificity: Current case definition does not have biomarkers, so Hepatitis A-E currently grouped together Non-viral hepatitis (e.g. alcohol abuse) may also be included • Validity: Limited financial and human resources for systematic implementation and quality assurance • Generalizability: Data only representative of symptomatic cases • Completeness: Severe underreporting # reported cases through surveillance < 20% of # estimated deaths through Global Burden Disease
Hepatitis and HIV case reporting Viral hepatitis HIV General Department of Preventive Medicine (MOH) Viet Nam Administration of HIV/AIDS Control (MOH) E-report Provincial Preventive Medicine Centre (63) Provincial AIDS Centre (63) E-report District (~1,100) Paper-based reporting Commune (> 10,000)
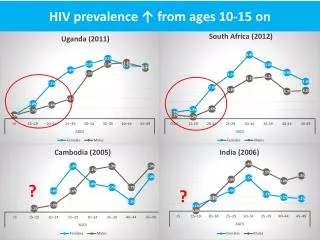
HIV Surveillance System • Vietnam has an HIV epidemic concentrated in: PWID, FSW, and MSM • System of HIV/AIDS case reporting (1992) in all 63 provinces. The first HIV positive case was detected in 1990. Cumulatively ~245,000 people living with HIV reported • Integrated Behavioral-Biological Survey (IBBS) was implementing 3 rounds (2005, 2009, 2013) among PWID, FSW, and MSM in 12 provinces of the most serious epidemic in Vietnam. Measures risk and preventive behaviors including sexual and drug-used behaviors as well as exposure to HIV/AIDS intervention programs • System of HIV sentinel surveillance - HSS (1994) (now reaches 40 provinces) in PWID, FSW, and MSM. HSS integrated with priority behavioral indicators (HSS+) started in 2010. Ministry of Health has guidance on national implementation through circular 9/2011/TT-BYT
Hepatitis Testing in IBBS • In the first two rounds of IBBS (2005 and 2009), only biological indicators from different populations were collected: • HIV prevalence • STI prevalence: syphilis, chlamydia, and gonorrhea • In IBBS III (2013), some more biological indicators were decided to add in for IBBS II and IBBS III: • CD4 count • Viral load • HIV drug resistance • HBV, HCV • Why hepatitis testing was added • Key populations at high risk for HCV and HBV transmission • HCV related liver disease become leading cause of mortality among those co-infected with HIV • No existing laboratory-based hepatitis surveillance
IBBS Hepatitis Methods - 2009 • Approximately 3000 PWID, 2500 FSW, and 1500 MSM tested for viral hepatitis in 2009 IBBS round • Algorithm for HBV testing:
IBBS Hepatitis Methods - 2009 • Algorithm for HCV testing:
IBBS Hepatitis Methods - 2013 • Approximately 1422 PWID, 1863 FSW, and 1266 MSM tested for viral hepatitis in 2013 IBBS round • Algorithm:
Conclusions • HIV prevalence were varied by provinces and by high-risk populations (highest in PWID, second in FSW, and third in MSM) • Proportion of HCV+/HIV+ in PWID was very high (91.1-97.2%) • Proportion of HCV+/HIV+ was highest in PWID (91.1-97.2%), MSM (90.0-98.5%), and FSW (22.9-72.5%) • Proportion of HCV+/HIV+ was always higher proportion of HBV+/HIV+ in all three populations • Proportion of HIV+/HCV was high in PWID (23.6-44.8%)
Recommendations • Study on HIV/HCV/HBV among general population will be needed • HBV/HCV surveillance system in high-risk populations need to be set up • ARV programme need to be urgently put HCV and HBV treatments in the programme
Lessons Learned from IBBS Advantages • Used existing surveillance system-> saves money from collecting new specimens • Good domestic capacity for serological testing allows identification of HBsAg and anti-HCV • Using existing staff and infrastructure from HIV surveillance was feasible for HBV and HCV Challenges • Requires substantial financial and human resources -> HSS may be more affordable than IBBS? • Procuring test kits come from different sources takes time -> Central procurement may be more efficient • Did not have enough equipment domestically for confirming chronic HCV infection with PCR -> maybe use DBS or Gene Xpert in future
Unresolved issues • Appropriate frequency for HBV and HCV surveys? • Focus populations? HCV burden largely mirrors HIV in key populations while HBV has higher prevalence in general population • Integration with existing efforts? HSS for key populations? General Statistic Office household surveys for general population? • Funding? Viet Nam government? Bilateral partners (e.g. US Government)? Global Fund? • Improving quality of case reporting data? Essential for measuring cascade of viral hepatitis services
Acknowledgments We would like to express our sincere thank to: • Supervisors, laboratory staffs of PACs, • Peer educators, other persons who worked in the surveys from participated provinces We especially thank to organizations who supported finance and technique to implementing the surveys: • CDC Atlanta and in Vietnam • Family Health International – FHI • Abbott company who supported a part of test kits for this study