Download
1 / 5
60 likes | 158 Views
AIDS Round1: Prevention (SR: PATH, TBCA, BATS-Prev, DPF, PDF, Raks Thai, YMAT ). Impact. To reduce incidence of HIV infection among youth. G1.1: HIV prevalence among male conscripts. G1.2: HIV prevalence among pregnant women aged < 25 years.

E N D
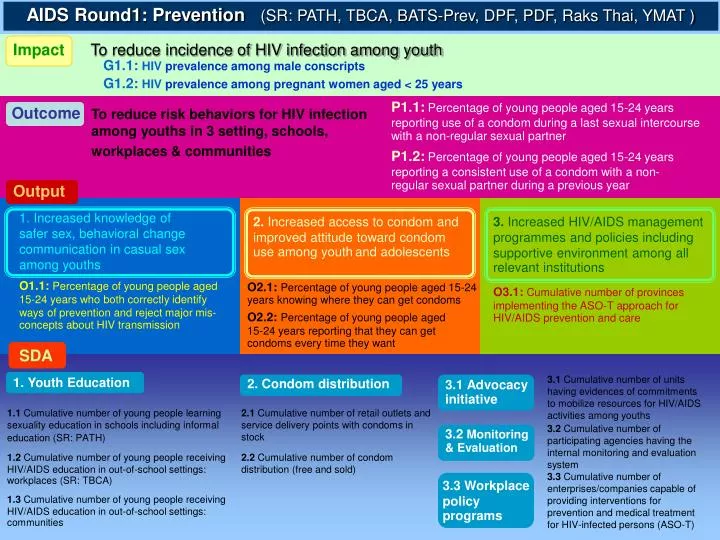
AIDS Round1: Prevention (SR: PATH, TBCA, BATS-Prev, DPF, PDF, Raks Thai, YMAT ) Impact To reduce incidence of HIV infection among youth G1.1:HIV prevalence among male conscripts G1.2:HIV prevalence among pregnant women aged < 25 years P1.1:Percentage of young people aged 15-24 years reporting use of a condom during a last sexual intercourse with a non-regular sexual partner Outcome To reduce risk behaviors for HIV infection among youths in 3 setting, schools, workplaces & communities P1.2:Percentage of young people aged 15-24 years reporting a consistent use of a condom with a non-regular sexual partner during a previous year Output 1. Increased knowledge of safer sex, behavioral change communication in casual sex among youths 2. Increased access to condom and improved attitude toward condom use among youthand adolescents 3. Increased HIV/AIDS management programmes and policies including supportive environment among all relevant institutions O1.1:Percentage of young people aged 15-24 years who both correctly identify ways of prevention and reject major mis-concepts about HIV transmission O2.1:Percentage of young people aged 15-24 years knowing where they can get condoms O3.1:Cumulative number of provinces implementing the ASO-T approach for HIV/AIDS prevention and care O2.2:Percentage of young people aged 15-24 years reporting that they can get condoms every time they want SDA 3.1 Cumulative number of units having evidences of commitments to mobilize resources for HIV/AIDS activities among youths 1.Youth Education 3.1Advocacy initiative 2.Condom distribution 1.1 Cumulative number of young people learning sexuality education in schools including informal education (SR: PATH) 2.1 Cumulative number of retail outlets and service delivery points with condoms in stock 3.2 Cumulative number of participating agencies having the internal monitoring and evaluation system 3.2Monitoring & Evaluation 1.2 Cumulative number of young people receiving HIV/AIDS education in out-of-school settings: workplaces (SR: TBCA) 2.2 Cumulative number of condom distribution (free and sold) 3.3 Cumulative number of enterprises/companies capable of providing interventions for prevention and medical treatment for HIV-infected persons (ASO-T) 3.3Workplace policy programs 1.3 Cumulative number of young people receiving HIV/AIDS education in out-of-school settings: communities
AIDS Round1: Care & Treatment (SR: BATS-Care, PHPT, HIV-NAT, ACCESS, NCA) Impact To reduce mortality and morbidity associated with HIV/AIDS G2.1:Percentage of PLWHA starting ARV still alive at 12 month P2.1: Cumulative number of PLWHA receiving ART under national program and GF grants Outcome To increase accessibility to ART, OI prophylaxis and expand sustainable comprehensive care and support for PLWHA P2.2: Percentage of PLWHA receiving OI prophylaxis as necessary 1) PCP 2) Cryptococcosis Output 4. Expanded and Increased comprehensive and continuum of HIV/AIDS care and support 5. Improved technical and health care system capacity 6. Supported and strengthened the PLWHA network so that their members have the necessary knowledge, skills and resources to participate as equal partners to response to HIV/AIDS effectively O5.1: Cumulative number of laboratories with capacity to monitor ART according to national guidelines: 1) CD4 2) Viral load 3) HIV resistance O4.1: Percentage of PLWHA who are still on treatment with good adherence after one year SDA 5.Information system & Operational research 4.1Treatment: ART and monitoring 6.1Supportive environment: Strengthening of civil society 4.1 Cumulative number of patients receiving ART under GF grants 6.1.1 Cumulative number of PLWHA outreach-worker groups carrying out activities in participating hospitals (groups) 5.2 Cumulative number of health care facilities implementing intervention on ART adherence 4.1 (new1) Cumulative number of patients under universal healthcare receiving laboratory service 5.3 Cumulative number of health care facilities implementing interventions on integrated VCT 6.1.2 Cumulative number of PLWHA outreach-worker groups carrying out activities in participating (persons) 4.1 (new2) Cumulative number of HIV/AIDS patients who are underprivileged and not eligible for health insurances received ART 5.4 Cumulative number of health care facilities implementing study on optimization of ART 6.2 Cumulative number of clients; HIV infected or not and/ or families affected by HIV/AIDS receiving care and support at holistic service points provided by trained PLWHAs 4.2HIV/AIDS care and support: Home based care 4.2 Cumulative number of people reachedby home-based care services (SR: NCA)
AIDS Round2 (ECAT: SR: DoH, TNAF) Impact / OutcomeII> To improve quality of life for HIV infected mothers, their partners and children 1.Percentage of HIV- infected persons who are still on antiretroviral (ARV) treatment after 12 months from the initiation of treatment 3.Percentage of children born to HIV-positive mother still alive at 12 month 4.Percentage of fully growth and developed children born to HIV-infected mothers 2.Percentage of HIV- infected mothers still alive at 12 months after delivery Objective 1. To increase capacity of public health personnel in the PMTCT program as well as NGO/ PLWHA to provide care for HIV-infected mothers, their partners and children 2. To provide comprehensive care and treatment intervention for HIV infected mothers and children 3. To assure that government policies and implementing agencies are providing appropriate support for HIV – infected women SDA 1.Supportive environment: Strengthening of civil society 2.1Care & Support for the chronically ill and their families 2.2 Treatment: ART and monitoring 2e. Cumulative number of HIV- infected migrant/stateless mothers whose CD4 < 200/mm3 or who are symptomatic that are receiving ARV treatment 2a. Cumulative number of HIV-infected mothers receiving continuous counseling and comprehensive care (SR: DoH) 1a. Cumulative number of Training of Trainers (TOTs) trained on ECAT (SR: DoH) 2f. Cumulative number of HIV- infected migrant/stateless partners of HIV-infected mothers whose CD4<200/mm3 or who are symptomatic that are receiving ARV treatment (SR: DoH) 1b. Cumulative number of counselors trained on disclosure and no ANC (SR: DoH) 2b. Cumulative number of HIV-infected mothers receiving counseling and comprehensive care (SR: DOH) 1c. Cumulative number of health stations personnel trained on comprehensive care for ECAT (SR: DoH) 2g. Cumulative number of HIV-infected migrant infants whose CD4<25% or who are symptomatic that are receiving ARV treatment (SR: DoH) 2c. Cumulative number of HIV-infected migrant/stateless mothers receiving counseling comprehensive care (SR: DoH) 1d. Cumulative number of health station personnel received program orientation dealing with migrant/ stateless groups (SR: DoH) 2d. Cumulative number of migrant/stateless partners of HIV-infected mothers receiving counseling comprehensive care (SR: DoH) 3.Supportive environment: Stigma reduction and respect of confidentiality 1e. Cumulative number of NGO staff and PLWHA trained on comprehensive care (SR: TNAF) 3a. Cumulative number of provinces implementing activities against stigma and for discrimination reduction (SR: DoH) 2h. Cumulative number of families of HIV infected mothers receiving psycho social support from the community, hospitals and sub-district health stations (SR: TNAF) 3b. Cumulative number of TAO supporting the activities against stigma and discrimination reduction (SR: TNAF) 2i. Cumulative number of children of HIV infected mothers receiving psycho social support from the community, hospitals and sub-district health station (SR: TNAF) 3c. Cumulative number of policy makers attending sensitization workshops (SR:DoH, TNAF)
Malaria Round2 Impact / Outcome To reduce malaria burden aiming at outreach population in high malaria areas in 9 provinces by working through home and community based activities under the support of local health sectors and local administrative organizations 1.Annual parasite incidence 2.Malaria death rate 3.Coverage of household owning ITN 4.Percentage of villages where at least 80% of population sleeping under bed nets Objective 1. To enable population in the targeted 300 villages to be aware of good health and be involved in home and community based activities for malaria control. 2. To increase the access to early detection and prompt effective anti-malarial treatment at the local health sectors as well as in the community. 3. To introduce insecticide treated nets (ITN) as a tool for protection from mosquito and reducing malaria transmission in the targeted areas. 4. To prevent the excess of malaria transmission in targeted areas through the establishment of malaria epidemic preparedness and control system. SDA 1.Prevention: BCC communication outreach 2.Treatment: Prompt, effective anti-malarial treatment 3. Prevention: Insecticide-treated nets (ITNs) 1a. Cumulative number of volunteers trained for BCC and malaria diagnosis and treatment 2a. Cumulative number of Malaria diagnosis and treatment posts established in outreached villages (Malaria Post) 3a.1 Cumulative number of ITN distributed and net re-treated with insecticide solutions 1b. Cumulative number of people reached by behavioral change communication activities 3a.2 Cumulative number of LLITN distributed 2b. Cumulative number of health workers at the district level trained in prompt and effective anti-malaria treatment 3b. Cumulative number of households owning an ITN or LLITN 2c. Percentage of patients with uncomplicated malaria getting correct treatment at health facility and community levels, according to national guidelines, within 24 hours of confirmation of symptoms 4. Information system & Operational research 4a. Cumulative number of districts with map showing high risk villages located in epidemic prone areas 2d. Percentage of health facilities reporting no disruption of stock of anti-malaria drugs and rapid diagnostic kits
TB Round 1 1. Prison [SR: DOC, BTB] 2. Border [SR: BTB, WVFT- Ranong, WVFT- Phang-nga, KRCH] 3. Urban [SR: BTB, ATAT- Chiang Mai, Srivichai 5 Hospital] 4. TB-HIV [SR: BTB, TBCA] To establish, expand WHO standard TB Care and Services to reach marginalized population and HIV infected persons in Thailand Impact / Outcome 2.Reduced number of smear-positive all form of TB cases per 100,000 population per year 1.Increase case detection rate 3.Increase treatment success rate Objective 3. Expansion of WHO standard TB case management with DOTS strategy to control TB in Urban Poor area in Thailand 4. Scale up and Expand HIV-TB care and prevention in high HIV prevalent provinces 1. Expansion of WHO standard TB case management with DOTS strategy to control TB prevent TB transmission in Large Prisons in Thailand 2. Expansion of WHO standard TB case management with TB strategy to control TB in border area and cross-border population in Thailand 1.Health system strengthening TB-HIV Prison Border Urban 1.1 Cumulative number of DOTS services, DOTS corner and TB clinic in prisons with adequate drug supply 2.Timely detection and quality treatment of cases 2.Timely detection and quality treatment of cases Prison Border Urban 1.2 Cumulative number of new smear positive TB cases detected 4.1 Cumulative number of provinces providing integrated AIDS-TB care S D A 1.3.1 Percentage of new smear positive TB cases registered under DOTS who are successfully treated Prison Border Urban 4.2 Cumulative number of HIV-TB coordinators and local staffs trained on integrated care 1.3.2 Percentage of new smear positive TB cases registered under DOTS who default Prison Border Urban 1.3.3 Percentage of new smear positive TB cases registered under DOTS who die 3. TB/HIV collaborative activities: Intensified case-finding among PLWHA Prison Border Urban 1.3.4 Percentage of new smear positive TB cases registered under DOTS who are transferred to another management unit and for which there is no treatment outcome information Prison Border Urban 4.3 Cumulative number of PLWHA receiving TB screening services 1.3.5 Percentage of new smear positive TB cases registered under DOTS who are smear positive 5 months or later after initiating treatment 4.4 Cumulative number of TB patients receive HIV counseling and testing Prison Border Urban