Download
1 / 42
420 likes | 586 Views
The Continuing Challenge of MRSA. Jim Thigpen, PharmD, BCPS Assistant Professor Bill Gatton College of Pharmacy. Disclosure Statement of Financial Interest. I, Jim Thigpen ,

E N D
The Continuing Challenge of MRSA Jim Thigpen, PharmD, BCPS Assistant Professor Bill Gatton College of Pharmacy
Disclosure Statement of Financial Interest • I, Jim Thigpen, DO NOT have a financial interest/arrangement or affiliation with one or more organizations that could be perceived as a real or apparent conflict of interest in the context of the subject of this presentation.
Disclosure Statement of Unapproved/Investigative Use I, Jim Thigpen, DO anticipate discussing the unapproved/investigative use of a commercial product/device during this activity or presentation.
Learning Outcomes • Describe the clinical presentation and diagnosis of MRSA • Classify the therapeutic options available for the treatment of MRSA • Formulate a therapeutic plan for the treatment of MRSA in various situations
A little history • Staphylococcus was first identified in Aberdeen, Scotland in 1880 by the surgeon Sir Alexander Ogston in pus from a surgical abscess in a knee joint • Staph is the most common isolated human pathogen • MRSA was first identified and coined in 1961 • Boston had the first U.S. outbreak in 1968 David MZ, Daum RS. ClinMicrobiol Rev July 2010, 616-687
A little more history • In 1975, 2.4% of Staphwere MRSA, by 1991, it was 29% • Into the ’90s, the term “MRSA” was used to describe infections in hospitals, other healthcare environments, and in their patients • Since the mid ’90s, there has been an explosion of MRSA in populations lacking risk factors for exposure to the healthcare system David MZ, Daum RS. ClinMicrobiol Rev July 2010, 616-687
What is MRSA? • Hospital-Acquired (HA-MRSA) • These strains carry a large staphylococcal chromosomal cassette mec (SCCmec) belonging to Type I, II, or III. They carry the mecA gene, which is nearly universal among MRSA isolates. • In HA-MRSA, the mecA gene usually confers resistance to most non-β-lactam antibiotics • Isolated largely from people exposed in a healthcare setting and are older with risk factors • More often causes PNA, bacteremia, and invasive infections David MZ, Daum RS. Clinical Infectious Diseases 2010;23(3):616-687
What is MRSA? • Community Acquired (CA-MRSA) • Carry smaller mec elements, most commonly SCCmec type IV or V. They also carry the mecA gene, but are more sensitive to non-β-lactam antibiotics than HA-MRSA • Frequently carry genes for Panton-Valentine leucocidin (PVL) • PVL is a leucocidin that can lyse the cell membrane of human neutrophils and may inactivate mitochondia • Shown to be dermonecrotic, possibly explaining the characteristic skin lesions associated with CA-MRSA David MZ, Daum RS. Clinical Infectious Diseases 2010;23(3):616-687
What is MRSA? • Community Acquired (CA-MRSA) • Carry Arginine Catabolic Mobile Element (ACME), which may help CA-MRSA colonize the skin of healthy people and spread • CA-MRSA usually affects a different population and causes different clinical syndromes • Previously healthy younger patients • Mainly SSTIs, but PNA and sepsis are also seen David MZ, Daum RS. Clinical Infectious Diseases 2010;23(3):616-687
The Challenge Continues • “escaped” or “feral” strains of HA-MRSA • Blended strains are even more resistant • In some regions, CA-MRSA accounts for 75% of Staph in children • Increased pressure on vancomycin has resulted in VISA and VRSA strains • MIC “creep” Clinical Infectious Diseases 2006;42 (Suppl 1) S40-S50.
Why has this happened? • CA-MRSA isolates occurred in the late ’90s in tandem with ↑ use of fluoroquinolones • No mechanism to link them • Elimination of MSSA strains from nasal mucosa? • CA-MRSA isolated occurred as routine childhood pneumococcal vaccines were introduced • CA-MRSA may have filled the niche left by Strep pneumoniae David MZ, Daum RS. Clinical Infectious Diseases 2010;23(3):616-687
Risk Factors • HA-MRSA • In the setting or has prior exposure • HD, surgery, LTCF resident, indwelling catheter • CA-MRSA • MRSA infection diagnosed within 48 hours of admission and without risk factors David MZ, Daum RS. Clinical Infectious Diseases 2010;23(3):616-687
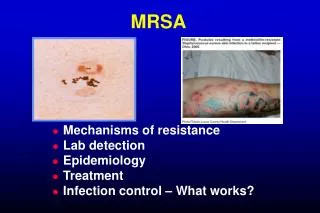
Clinical Manifestations • Skin and soft tissue infections (SSTIs) account for up to 95% • Often look like a spider bite • Cellulitis may typically develop on unbroken skin • Septic arthritis, osteomyelitis and pyomyositis are most common invasive infections in kids David MZ, Daum RS. Clinical Infectious Diseases 2010;23(3):616-687
Treatment • Skin and Skin Structure Infections (SSTIs) • Incision and drainage is primary treatment • Clindamycin vs Cephalexin showed equal efficacy when treating an uncomplicated SSTI† • Nearly all children had active or passive drainage of purulent collections before antibiotics were started • Higher rates of recurrent SSTIs have been reported within 10 days in a study comparing SMX/TMP to placebo‡ † Chen AE, Carroll K, et al. Pediatrics 2011;127;e573 ‡ Duong M, Markwell S et al. Ann Emerg Med. 2010;55(5):401-407
Treatment • Skin and Skin Structure Infections (SSTIs) • Antibiotic therapy is recommended for abscesses associated with the following conditions: David MZ, Daum RS. Clinical Infectious Diseases 2010;23(3):616-687
Treatment • Skin and Skin Structure Infections (SSTIs) • Cellulitis with purulent drainage (cannot be drained) • Oral clindamycin, SMX/TMP, doxy- or minocycline, or linezolid • Cellulitis with non-purulent drainage • Think β-hemolytic strep (penicillin or cephalexin) • If unresponsive to β-lactam or systemic toxicity present, then cover CA-MRSA also with clindamycin alone, SMX/TMP or tetracycline in combination with amoxicillin, or linezolid alone • 5 – 10 days of therapy • Use of rifampin as a single agent or adjunct is NOT recommended David MZ, Daum RS. Clinical Infectious Diseases 2010;23(3):616-687
Treatment • Skin and Skin Structure Infections (SSTIs) • For hospitalized ADULT patients with complicated SSTIs (deeper, surgical or traumatic wound infections, major abscesses, cellulitis and infected ulcers or burns), in addition to surgical drainageand broad spectrum antibiotics, MRSA therapy should also be added pending culture results • IV vancomycin • PO or IV linezolid • IV daptomycin • IV or PO clindamycin • IV telavancin • 7 to 14 days of therapy David MZ, Daum RS. Clinical Infectious Diseases 2010;23(3):616-687
Treatment • Skin and Skin Structure Infections (SSTIs) • For CHILDREN with minor skin infections (impetigo) and secondarily infected skin lesions, mupirocin 2% can be used • In HOSPITALIZED children • IV vancomycin (15 mg/kg/dose q6h, with TDM) • If stable without ongoing bacteremia or intravascular infection, IV clindamycin (40 mg/kg/day q6-8h) if resistance is low, if strain susceptible, switch to oral • Linezolid (10 mg/kg/dose q8h PO/IV, or adult dose if ≥ 12) • 7 to 14 days of therapy David MZ, Daum RS. Clinical Infectious Diseases 2010;23(3):616-687
Treatment • MRSA Bacteremia (adults) • Uncomplicated bacteremia (+ cultures and NO endocarditis, no implanted prostheses, follow-up cultures at 48-96 hours do not grow, AF in 72 hours and no other evidence of infection) • Vancomycin or daptomycin • 14 days of therapy David MZ, Daum RS. Clinical Infectious Diseases 2010;23(3):616-687
Treatment • MRSA Bacteremia (adults) • Complicated bacteremia • Vancomycin • Daptomycin 6 mg/kg once daily, some recommend 8-10 mg/kg once daily • 4 – 6 weeks of IV therapy • Addition of gentamicin to vancomycin is NOT recommended • Addition of rifampin to vancomycin is NOT recommended David MZ, Daum RS. Clinical Infectious Diseases 2010;23(3):616-687
Treatment • MRSA Bacteremia (children) • Vancomycin for 2 – 6 weeks • Daptomycin 6-10 mg/kg once daily is an option • Not a lot of evidence • Clindamycin or linezolid should not be usedif there is a concern for endocarditis or if an endovascular source of infection is suspected • Data supporting the use of rifampin or gentamicin is insufficient, choice to use is individualized David MZ, Daum RS. Clinical Infectious Diseases 2010;23(3):616-687
Treatment • MRSA Pneumonia • For HA-MRSA or CA-MRSA • IV vancomycin • IV/PO linezolid • IV/PO clindamycin • 7 – 21 days therapy David MZ, Daum RS. Clinical Infectious Diseases 2010;23(3):616-687
Treatment • MRSA Pneumonia (children) • IV vancomycin • IV clindamycin • if resistance rate is low • IV/PO linezolid 600 mg q12h for ≥ 12 years • IV/PO linezolid 10 mg/kg/dose q8h David MZ, Daum RS. Clinical Infectious Diseases 2010;23(3):616-687
Treatment • MRSA Bone and Joint Infections (adults) • IV vancomycin • Daptomycin • TMP/SMX 4 mg/kg/dose q12h + rifampin 600 mg daily • Linezolid • Clindamycin • Some experts recommend rifampin to all of the above, started after bacteremia has cleared • 8 weeks of therapy for osteomyelitis, 3-4 weeks is usually sufficient for septic arthritis Healthtap.com David MZ, Daum RS. Clinical Infectious Diseases 2010;23(3):616-687
Treatment • MRSA Bone and Joint Infections (children) • IV vancomycin • IV clindamycin • If stable and clindamycin resistance is low • IV Daptomycin • IV Linezolid • 4 - 6 weeks of therapy for osteomyelitis, 3-4 weeks is usually sufficient for septic arthritis David MZ, Daum RS. Clinical Infectious Diseases 2010;23(3):616-687
Treatment • MRSA infections in the CNS • Vancomycin + rifampin • Linezolid • TMP/SMX 5 mg/kg/dose q8-12h • Clindamycin does not penetrate the CNS • Meningitis – 2 weeks • Abscess, etc – 4 to 6 weeks • Vancomycin for pediatrics David MZ, Daum RS. Clinical Infectious Diseases 2010;23(3):616-687
Adjunctive Therapies • Clindamycin and linezolid are NOT routinely recommended as adjunctive therapy for the management of invasive MRSA disease • The use of adjunctive IVIG is not recommended • Some experts may consider these agents in selected situations David MZ, Daum RS. Clinical Infectious Diseases 2010;23(3):616-687
Vancomycin Dosing • Adults • 15 – 20 mg/kg/dose (actual body weight) q8-12h, NTE 2 grams/dose is recommended with normal renal function • A loading dose of 25-30 mg/kg may be considered in seriously ill patients • Loading doses and larger doses should be infused over 2 hours to minimize “red-man” reaction • diphenhydramine David MZ, Daum RS. Clinical Infectious Diseases 2010;23(3):616-687
Vancomycin Dosing • Adults • For most patients with SSTI who have normal renal function and are not obese, traditional doses of 1 gram q12h are adequate and serum levels are not required • For serious infections (bacteremia, endocarditis, osteo, meningitis, PNA, and severe SSTI, vancomycin trough levels of 15 – 20 mcg/ml are recommended David MZ, Daum RS. Clinical Infectious Diseases 2010;23(3):616-687
Vancomycin Dosing • Why do we need these levels? • AUC/MIC best relates to antibacterial effect of vancomycin • (AUC24)/MIC of ≥ 400 is the target • This number can be achieved with trough levels of ≥ 15 mcg/ml • When is this really important? • MIC of vancomycin is > 1 mcg/ml • More severe infections
Vancomycin Dosing • What is the risk? • There is an increased risk of nephrotoxicity seen with vancomycin where troughs are > 15 mcg/ml¥ • Nephrotoxicity was defined as a rise in serum creatinine of 0.5 mg/dl or a >50% increase from baseline level for two consecutive labs • An incidence of 29.6% was observed when trough levels exceeded 15 mcg/ml • What does this mean to us? ¥ Bosso JA, Nappi J, et al. Antimicrobial Agents and Chemotherapy 2011;55(12):5475-9
Treatment Alternatives(when MRSA won’t clear or vanco fails) • High dose daptomycin (10 mg/kg/day) in combination with gentamicin 1 mg/kg IV q8h, rifampin, linezolid, or TMP/SMX • If reduced susceptibility to vancomycin or daptomycin are present, quinupristin/dalfopristin, TMP/SMX, linezolid or telavancin should be considered either alone or in combination David MZ, Daum RS. Clinical Infectious Diseases 2010;23(3):616-687
What else do we have? • Tigecycline • Protein synthesis inhibitor “souped-up doxy” • Low serum levels and probably not effective for pneumonia limit it’s use • Quinupristin/dalfopristin • Protein synthesis inhibitor • Frequent side effects, drug interactions, limited data in severe disease
What else do we have? • New Lipoglycopeptides • Developed by altering the structure of vancomycin • Added a lipophilic “tail”, increasing the antimicrobial activity, and a hydrophilic moiety, improving the pharmacokinetics • Telavancin (VIBATIV®) • Dalbavancin • Oritavancin Zhanel GG, Calic D, et al. Drugs 2010;70(7):859-886
What else do we have? • Telavancin (VIBATIV®) • Two mechanisms of action • FDA approved for SSTIs, HAP • Non-inferiority trials with vs vancomycin • Some concerns with nephrotoxicity • Not as effective in patients with CrCl < 50 • Pregnancy test (problems in animal models) • Active against VISA, not VRSA Zhanel GG, Calic D, et al. Drugs 2010;70(7):859-886
What else do we have? • Dalbavancin (investigational) • Effective for SSTIs • Once weekly dosing due to long half-life • Oritavancin (investigational) • May be dosed once for the course • May also be effective vs VRSA Zhanel GG, Calic D, et al. Drugs 2010;70(7):859-886
What else do we have? • Fusidic acid • A protein synthesis inhibitor • Has been used effectively across the globe • “Resurrected” for use in the U.S. • Less active vs β-hemolytic strep • Oral availability Moellering, R, Corey G. Clinical Infectious Diseases 2011;52(S7):S467-S468
What else do we have? • Ceftaroline (Teflaro®) • FDA approved for CABP (Strep pneumo) and SSTIs (MRSA) • Not as effective vs resistant gram-negatives • Ceftibiprole (investigational) • MRSA activity, gram-negative activity similar to cefepime • Tedizolid (investigational) • Shorter course and fewer side effects
Learning Outcomes • Describe the clinical presentation and diagnosis of MRSA • Classify the therapeutic options available for the treatment of MRSA • Formulate a therapeutic plan for the treatment of MRSA in various situations