Breakthroughs in Operating Room Efficiency
Breakthroughs in Operating Room Efficiency. Presented by Dr Terry Loughnan Director of Anaesthesia. Why?. Internally recognised that improving the performance of operating theatres is a key to improving services for patients.

Breakthroughs in Operating Room Efficiency
E N D
Presentation Transcript
Breakthroughs in Operating Room Efficiency Presented byDr Terry Loughnan Director of Anaesthesia
Why? • Internally recognised that improving the performance of operating theatres is a key to improving services for patients. • Independent Review in 2003 concluded that there were gains to be made within existing resources. (Giffney Report)
Why? • Emerged from specialist survey in June 2004 that operating room efficiency was the highest priority improvement opportunity.
Our Objectives • Maximise utilisation of current theatre resources • Reduce time lost due to late starts and changeover • Reduce Cancellations • Increase patient throughput • Improve Satisfaction of Patients, Specialists, OR Staff
Scope Four Procedural Areas across 2 sites Rosebud • 1 Theatre for Low risk patients undergoing elective surgery excluding joint replacements and laparotomies Frankston • Day Surgery Unit (free standing) • Endoscopy Unit (separate to Main Theatre) • Theatre Suite of four operating rooms
Our Team • Director of Anaesthesia (Project Manager) • Executive Director Medical Services • Director of Surgery • Orthopaedic Surgeon (VMO representative) • Consumer Representative • Operations Director Surgery and Inpatient Services • Nurse Managers of the 4 Procedural Areas and Admission/Discharge Lounge • Consultants and Six Sigma Facilitator • Manager Admissions/Discharges • Project Officer • ESAC Coordinator
Project Plan • Establish Structure of Team • Define Project • Measure Current Situation • Complete Analysis • Plan and Trial Improvements • Control/Redesign Process • Evaluate and Review Project
Methodology Six Sigma Improvement Process • Define • Measure • Analyse • Improve • Control • Structured approach with emphasis on appropriate quality tools.
Meetings • Initially every second Monday morning at 0800 – 0930. • Located away from Operating Suite. • Activities have generated free flowing discussion and far greater understanding of the challenges faced in other areas.
Quality Tools • Affinity Diagram (brainstorming session of relevant issues) • Value Chain/Process Mapping • Critical to Quality Analysis • Survey of Issues by Site • Cause and Effect Diagrams
Data Collection Issues Identified by Site
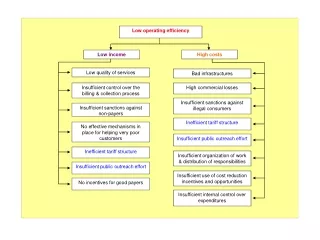
Cause & Effect Diagram: Cancellations on the Day Processes/Procedures Equipment Staff/People ‘Fasting’ guidelines/usednot understood by patients (use ‘nil by mouth’) Illness - Sick staff Bed unavailability:- ICU/general beds Unavailability Overruns Staff attitude • not working out of hours • safe working hoursrequired Breakdown Staff unavailablebetween 4.30pm and 6.00pm/safe hours Scheduling to fill the time &emergency cases intervene Rostering(safe hours) Poor planning for/booking of appropriate equipment Lack of an emergency theatre Non-worked up patients Surgeons/staff on holiday and PH not notified Delayed starts Effect Poor bed availability Causes Cancellations on the day Inappropriate health questionnaire screening (for day theatre) through PAC, eg. Anaesthetists miss pieces of information (patient completed questionnaire) Poor bed availability data Pathology equipment/staff unavailable/inappropriate on the day Undiagnosed, sickpatient (acute illnessafter preparation) Poor predictive data re length of operations& equipment required We don’t know whether beds available Emergencies - management & semi- urgent cases No real time data rein-patients for theatrewho are fasting/nil bymouth Equipment breakdown Overruns Technology Data Environment
Cause & Effect Diagram: Delays in Theatre Staff/People Processes/Procedures “Late culture” • Everything runs a little late • - No expectation to start ‘on time’ • Surgeons bookings from other hospitals Processes reliant on surgeon (who didn’t start on time) How do we know when surgeons due? Surgeons don’t want to wait around/be kept waiting with patients not ready Poor patient discharge Medical, education teaching- scheduled deferred starts - skills mix Start times do not relate to surgeons Are we scheduling to give surgeons enough time? • lists are too full • all day lists at Rosebud/one site? Poor booking of eg. Pacemaker technician Staff availability/absenceseg. Monday technician(sick leave) No “team driver”- surgeons are key in the process Effect Causes Unplanned delays, late starts Poor forecasting ofequipment required Poor CSSD capacity & logistics: need a quicker cycle Poor knowledge of accurate list Arthroscopy need digital equipment increasingly Theatre staff have to wait for surgeons People work on other things & are legitimately late Machines being sent between sites, eg Endoscopy equipment not available until 9.00am On time theatre not a priority Poor data re wards/ ICU status (& beds), post 9.30am meeting Overrun of other lists earlier in the day causes delays Impact of emergencies Poor predicted times of length of operation- compounds as the day goes on Poor parking for staff Morning/night theatre overruns Technology Data Environment
Challenges • Christmas break and Public Holidays. • Availability of Visiting Medical Officers (VMOs). Everyone is willing to be involved but no-one can attend a meeting. • Shortened time-lines and need to start . • Avoiding use of the word “Efficiency”.
Successes • Discovering the true functions of our procedural areas. eg Admission and Discharge Lounge
Communication Letters to all • surgeons • endoscopists • other proceduralists Regular contact with VMO representative
Current Activities • Data Collection Rosebud Operating Suite Frankston Operating Suite Frankston Endoscopy Frankston Day Surgery • Surgeon Interviews • Focus Groups
Data Collection Simple forms specific to each area Compatible with NHS Definitions Common Data Items: examples • Times of arrival of Surgeon • Times of arrival of Anaesthetist • Time patient called for by OR • Time patient sent to OR from preparation area • Time induction commenced • Time “knife to skin” • Time transferred to recovery • Time ward called to collect patient • Time patient left recovery
Surgeon Interviews • Surgeons from each specialty were nominated by Director of Surgery • Letter sent to all surgeons with list of suggested interviewees • Those not on the list were invited to make contact if they wished to be interviewed. • Appointment times and locations scheduled to suit surgeon
Surgeon Interviews • Quantify expectations of the surgeons regarding issues such as Knife to skin time, • Perceptions of current performance of the Theatre • Suggested improvements within current resources
Focus Groups • Patients • Anaesthetists/Registrars • Surgeons/Registrars • Theatre Nursing Staff (both day and evening groups) • Theatre technicians/PSAs/Reception Ideally 8-9 participants for 40-50 minutes Letter to staff to explaining process and inviting them to participate
Planned Future Activity • Process re-design workshop. To be held in the evening with interested stakeholders to review the data collected and address issues raised, to improve theatre utilisation. Aim is to have stakeholders re-design the process to meet the customers expectations.