Download
1 / 13
130 likes | 272 Views
Coronary Artery Bypass Grafting in Awake Settings. Mitrev Z , Anguseva T. Special hospital for Cardiosurgery “Filip II” Skopje - Macedonia. Myocardial revascularisation in awake patients:. 1.Avoidance of extracoropreal circulation,

E N D
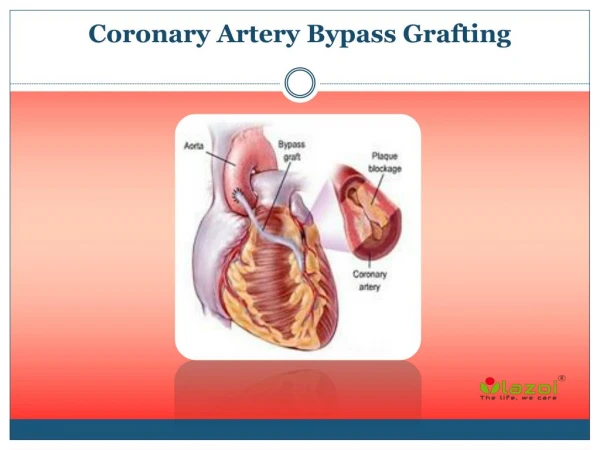
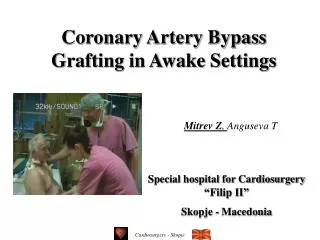
Coronary Artery Bypass Grafting in Awake Settings Mitrev Z, AngusevaT Special hospital for Cardiosurgery “Filip II” Skopje - Macedonia
Myocardial revascularisation in awake patients: 1.Avoidance of extracoropreal circulation, 2.General anesthesia, endotracheal intubation and mechanical ventilation unnecessary 3.Complete off-Pump revascularisation possible
Material and Metods High epydural analgo-anesthesia N= 10 pts ( 2 femail, 8 mail) - Epidural catheter in place: Th1-Th2 - Main targed: somatosensory and motor block - Applied medicaments: 20ml 0.25%Bupivacain 100gr.Fentanyl, 5ml/min - Sternotomy: patient being without intubation - CABG
Schematic view The catheter is placed in the high epidural space Th1-Th2 one day preoperatively, using the loss of resistance method, or method of getting a drop
Patient demographics (N : 10) • Age (years) 62.2 ± 7.8 • Sex (f/m) 2/8 • BSA (cm2) 1.76 ± 0.2 • Unstable angina n : 5pts • Previous myocardial infarction n : 4pts • Coronarography finding Comorbidities: • LAD 100% (n : 10) Hyperlipidemia – 7pts • LAD 100%; Cx 90% (small) Diabetes disease- 4pts • (n:2) Hypertension – 8pts • COPD – 2pts • Adiposity – 1pts • Smokers – 6pts
Management procedures • First step: epidyral catheter the day before surgery • Second step: The operative day-.Analgosedation with: mixture 1 :0.5% Bupivacain and 1.66g/ml Su-Fentanyl – starting at sternotomy till sternal rewiring mixture 2 : 0.125%Bupivacain and 1 g/ml Su-Fentanyl Day 1 to 3 after surgery • Dosage of the analgosedativa is correlated with: Pts haemodynamic stability Blood-gas analyses Visual analgoscala. Target: pain index 1to3 Third step: Postoperative analgosedatia with mixture 2 (first day)
Postoperative management • Third step: Postoperative analgosedatia with mixture 2 (first day) • Epidural cathether pull out after 24 hours • No need of cathecholamine support • No need of other additional sedation except epidural mixture 2 (0.125%Bupivacain and 1 g/ml Su-Fentanyl)
Results I –intraoperative data • Complete sternotomy 10 pts • CABG x1 (LITA - LAD) – 10pts • Mean time of bypassing 7.9±0.8min • Mean time of op.duration 71.7 ± 22.1min • Without intubation 9pts • 1patient intubated after sternotomy: pain index >7 • Entered left pleural spaces 2 pts • Hemodynamical stability in 10 pts
Results II-ICU events • Two patients left the operating room by walk. • Drains were pull out first post op. day in all pts • Hemodynamical stability 9pts • In hospital stay 2,5days 9pts • Without any significant postop. Complications • Follow up – 2 – 42months
Complications: • Perforation of the internal dura (1) • Intensive headache after punction of the dura interna (1) • Collaps due to the Puncture (2) • Radicular pain and back pain (7) • Epidural catheter misplacement (2) The risk of od epidural-spinal hematoma - decreased, following the recommendations of DGAI: --atraumatic inplacement -- appropriate interval of the last anticoagulant therapy
AWAKE SURGERY • Respiratory and haemodynamic stability • Decreased stress • Good ( pre-and postoperative ) Analgesie • Early mobilisation possible • Quick and effective recovery • Better economic side with a exellent clinical outcome