Coronary Artery Bypass
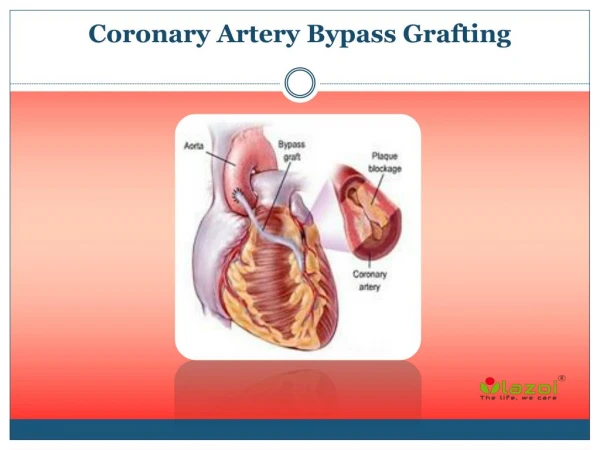
Coronary Artery Bypass . By: Brittney Mathis RN, BSN. Veins Used for Bypass. Saphenous vein -> Right Coronary Artery and Circumflex Internal Mammary Artery-> Left Anterior Descending Coronary Artery Patency over 90% after 10 years

Coronary Artery Bypass
E N D
Presentation Transcript
Coronary Artery Bypass By: Brittney Mathis RN, BSN
Veins Used for Bypass • Saphenous vein -> Right Coronary Artery and Circumflex • Internal Mammary Artery-> Left Anterior Descending Coronary Artery • Patency over 90% after 10 years • If more are needed, upper extremity veins can be used but patency is less than 40% after 5 years
Preoperative • Explain the lines that will be in place after surgery-ET tube, ART, Cortis, chest tubes, Foley • Explain use of IS following surgery and its importance. Go ahead and practice • Educate on proper body mechanics and sternal precautions that will be used for 6-8 weeks. Go ahead and practice. • Chest and both legs are to be shaved completely • The night before and morning of surgery, patient is to take a chlorohexadine bath and swish/swallow
Intraoperative Care Video of Bypass
Immediate Postoperative • Connect patient to proper monitors • STAT CBC, PT, PTT, BMP, MG, ABG, and glucose • STAT EKG, CXR • Connect chest tubes to suction and MONITOR CHEST TUBES: q15mins for 1 hour and then hourly. Call physician if output >150 mL first hour or >100 mL/hr thereafter • If it is greater, draw STAT PT/PTT, CBC, and Fibrinogen and call surgeon • Vitals signs every 15 minutes, including CVP, PA, CO/CI, and SVO2. Record an SVR every 4 hours or so, you may need to look up how to calculate it.
Calibrating Vigilence See Handout
Volume • Patient CVP needs to 7-12 mm Hg for hearts. • CI >2.2 • If these are low=patient needs volume • This allows a proper amount of volume to keep the new grafts open and patent • Standing orders for volume: 1Liter NS, 1 Liter Albumin (start with this), and sometimes 1 Liter of Hesban (don’t give if actively bleeding) • Can give one unit of PRBC if Hgb<8
Blood Pressure Control • MAP is usually to be kept between 65-75 • A MAP greater than 75 puts the patient at risk for rupturing a bypass suture and increases bleeding (chest tube output) from the suture line. • There will always be either Cardene, Nitroglycerin gtt, or sometimes Nipride ordered • If the patient systolic blood pressure is less than 90 and not responding to volume, call physician.
Electrolyte Replacement • Potassium is to be kept >4.0 mmol/L • Magnesium is to be kept >1.8 • Calcium is to be kept >8.5 • If at any time a CV surgeon rounds and these are not correctly, I can guarantee him to get angry.
Sign of Tamponade • Tamponade is the filling of the pericardium with fluid, pus, or blood. • This can happen if bypass was not stitched well and the chest tubes cannot drain fast enough or the chest tubes are not patent • Signs: increased CVP above PA pressures, decreased BP, increased HR, muffled heart sounds, pulsus paradoxus, and decreased CO/CI
Extubation • There is a Cardiac Weaning Protocol for Fast track. • Best Practice: extubated in 6 hrs, OOB in 2 hours • Criteria-no acute ischemia, hemodynamically stable, absence of new arrhythmia, blood loss <2 mL/kg.hr, awakening from anesthesia (following commands and lifting head off pillow), core temp >97.0 F 1. Pt placed on CPAP 2. ABG in 30 mins 3. NIF and VC 4. Call anesthesiologist for orders
Sternal Precautions These are to be followed for 6-8 weeks to allow proper healing of the sternum. • Do not lift more than 5-8 pounds. (Roughly a half gallon of milk) • No pushing or pulling with your arms. • Do not reach behind your back or reach both arms out to the side. • Do not reach both arms overhead. • Brace sternum with pillow while getting up, sitting down, coughing, and sneezing. Failure to follow these directions can result in sternal wires breaking and a surgical procedure to fix them will be needed.
Post Extubation Respiratory Care • Incentive Spirometer is to be done a minimum of 10 times every hour • Coughing and deep breathing (use sternal precautions) • Proper analgesics (promote deep breathing) • Early ambulation All of these decrease the risk for postoperative pulmonary complications that include: pneumonia and atelectasis.
Aminocaproicacid (Amicar) • AntifibrinolyticAgent-minimizes bleeding and decrease need for transfusion • Dose: • Monitor: incision sites for bleeding and chest tubes for clots
nicardipinehydrochloride (Cardene) • Mechanism of Action: calcium channel blocker than inhibits calcium ions from entering cardiac and vascular smooth muscle cells. causes arteries to dilate and blood pressure to decrease • Use: decrease BP, Increase CO, decrease SVR • Dosage: premixed bag of 40 mg in 200 mL. recommended starting dose at 5 mg/hr for max dose of 15mg/hr • Can be mixed in pharmacy for higher concentration on CRRT patients (Cardene I.V., 2013)
Nitroglycerin • Dosage: 5 - 200 mcg/min • Must be mixed in glass bottle & administered is special tubing
Sodium Nitroprusside(Nipride) • Mechanism of Action: Relaxes vascular smooth muscle to reduce afterload & preload • Use: decrease blood pressure • Dosage: 0.5 - 8 mcg/kg/min • Precautions: Protect from light and monitor serum Thiocyanate levels. Nipride metabolizes to cyanide. Cyanide toxicity can develop within 1 hr with infusions >10 mcg/kg/min
Milrinone (Primacor) • Phosphodiesterase inhibitor; positive inotrope with little chronotropic effect; direct vasodilator (decreases both preload & afterload) activity • Uses: heart failure • Dosage: Load: 50 mcg/kg IVP over 10 minutes. Then 0.375-0.75 mcg/kg/min IV infusion ("Medscape Reference," 2013)
Phenylephrine (Neosynphrine) • Mechanism of Action: Strong alpha effects resulting in increased peripheral vascular resistance and blood pressure; decreases cardiac output and renal perfusion • Use: Severe hypotension or shock • Dosage:20mg/250ml D5W at 100-180 mcg increments IV bolus, THEN 40-60 mcg/min continuous IV infusion • Side effects: pulmonary edema, V-tach, metabolic acidosis
DobutamineHCl (Dobutrex) • Mechanism of Action: inotropic agent whose primary activity results from stimulation of the b-receptors of the heart • Use: Increase contractility and CO in heart failure • Dosage:2.5 -10 mcg/kg/min • Warnings: may precipitate or exacerbate ventricular ectopic activity • Weaning: 1mL/hr, weaning too quickly can cause arrhythmias
References Milrinone. (2013). Retrieved June 11, 2013, from http://reference.medscape.com/drug/milrinone-342433#0 Cardene I.V. (2013). http://www.cardeneiv.com/c1_cardeneiv_ov.shtml