Human Resource Development a Step - Wise Approach - Indonesia
220 likes | 236 Views
This presentation discusses the country situation, health facilities related to TB control, background of the Dutch-supported project on HRD, objectives, preparatory phase, curriculum and training methodology, organization structure, mid-term external review, and impact.

Human Resource Development a Step - Wise Approach - Indonesia
E N D
Presentation Transcript
Human Resource Development a Step - Wise Approach - Indonesia DEWG Meeting, The Hague, 7-8 Oct ‘03
Country Situation • Population 217Million • Island 17,000 • Provinces 30 • Districts 357 • Sub-districts 4,069 • Villages 64,367 • Health Centers 7,200 • Hospitals 1,100 • GDP(per capita) $449 23% pop. live below poverty line • 60% Pop. Live in 7% land area (Java) = Makassar = Malang = Ciloto = Padang
Health Facilities related to TB Control • Health Center 7.312 • Microscopic Health Center 2.612 • Chest Clinic 34 • Provincial Health Laboratory 26 • HOSPITAL : • Lung Hospital (RSTP) 9 • District General Hospital 340 • Provincial General Hospital 40 • Private General Hospital 600
Back Ground • WHO External review mission in Feb 2000. • Major constraint identified was low level of knowledge & skills of staff at all levels. • This was related to the poor quality of training conducted in the past – material, methods & motivation. • To address this problem a proposal was developed for funding by the Dutch Govt to cover a period of 3 yrs 2000-2002 for a total of 5 M US $.BNE till 2003
Objectives of the Dutch Supported Project on HRD • To improve the quality of services delivered to TB patients through improvement of the skills of health workers at the various levels. • To improve the efficiency & cost-effectiveness of program management for leprosy & TB control in leprosy endemic areas.
Preparatory Phase • Review of all available training material. • Updating & revision of national guidelines for TB. Updating of Job descriptions – mid 2000. • Development of training curriculum for different levels – 3rd qtr 2000. • Trg curriculum for master trainers. • Trg curriculum for Prov & dist staff. • “ “ For UPK (HC) staff. • “ “ For lab technician’s. • Course director guide – UPK level. • Facilitator guide – UPK level.
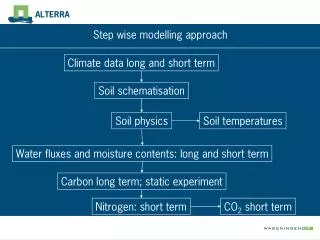
Training System Model PERFORMANCE DEFICIENCY Standardization TNA TRAINING OBJECTIVE TRAINING DESIGN TRAINING MONEV Implementation PRE PA RATION IN PUT PRO CESS OUT PUT OUT COME IM PACT MONITORING EVALUATION FOLLOW-UP / POST TRAINING EVALUATION
Curriculum & Training Methodology • Curriculum was based on job description, with more emphasis on practical exercises (60/40 P/T). • Teaching approach was based on the active learning & problem based learning approach. • Duration – MT 2 months; P & D 12 days; UPK initial trg 7 days & ref trg 3 days. • Batch size maximum 22 participants. • Ratio 1 facilitator/5 participants.
Core Group of Master Trainers • Committee est. For selection & recruitment of MT – mid 2000. • 23 MT recruited – 4th qtr 2000. • MT trained in Jakarta for 2 months by WHO Nat consultants, KNCV, Trg coordinator WHO HQ – Dec 2000/Jan’01. • 4 regional trg centers were selected to act as regional TB trg centers.
Core Group of Master Trainers • 4 centers are: – Makassar (N & E 10 Prov) • Malang (central 6 Prov) • Ciloto (central 5 Prov) • Padang ( west 9 Prov) • MT posted to the 4 centers in April 2001 • Trg for Prov & dist staff started – April ’01 to Feb ’02 • Total Prov & Dist supervisors trained - 948 • Trg of UPK & lab staff, march ’02 & ongoing (2500 UPK 35% & 1000 Lab 38% trained ‘01-’02)
TRAINING MANAGEMENT FACILITATOR TC Training Organization DG CDC&EH CENTRAL NTP MANAGER TECHNICAL SUPPORT TEAM PMU NATIONAL TRAINING COORDINATOR PROVINCE PROVINCIAL TB MANAGER TRAINING TEAM PPO PROVINCIAL TRAINING COORDINATOR TRAINING CENTER MANAGEMENT FACILITATOR TARGET (TRAINEE)
Mid Term External Review • External review done in Nov/Dec ’01. • Efforts made on trg related objectives were commendable. • Great enthusiasm shown in preparation phase & output good. • The 1st & 2nd phases of training on schedule & implemented well. • Contents & methodology, perceived as very satisfactory by participants & facilitators. • Implementation of the UPK trg was seriously delayed.
External Review Mission Jan ‘03 • External Program review done in Jan/Feb’03. • Remarkable progress made in last 2 yrs • Management of trg at central level strengthened • 26 specific recommendations made in Dec ’01, 19 implemented & others being addressed. • Little follow up on post training activities • Implementation of the UPK trg delayed, however momentum increasing with scaling up of activities in 2003.
Impact • Core group of MT established & functional. • Cadre of trainers established in all provinces. • Facilities upgraded for TB training in all 4 regional training centres. • Scope of MT expanded in Oct ’02 to national TB facilitators at Prov level. • Dutch project can cover only 20% HC staff. • TBCTA, CIDA & GFATM will cover the remaining gap.
Lessons Learnt (1) • Assign focal point for training within the NTP • Review of existing capacity based on task analysis and functions • Review existing training programmes and training material • Revise/develop task and level specific training material for skills development • Prepare a cadre of master trainers/facilitators • Organization of training courses (training plan) • Implement training plan • Monitor implementation and adjust plans as necessary • Supervise (identify staff turnovers and performance problems) and organise continuous education • Update pre-service training programmes for all categories
Lessons Learnt (2) • Technical assistance - short term and long term is essential for success • Earmarked financial resources facilitated the step wise process • Biggest constraint faced are in organizational aspects & bureaucracy, which leads to delayed disbursement of funds & subsequent delays in implementation