Download
1 / 58
600 likes | 683 Views
Learn about Mallet Finger, Trigger Finger, and Boutonniere Deformity, common hand deformities. Understand their causes, symptoms, management, and treatments, including splinting, surgery, and injections.

E N D
Hand Deformities, Fractures, and palsy By Adnan AL-Maaitah http://hastaneciyiz.blogspot.com Medical ppt
NOTE • The following subjects are NOT mentioned in the guidelines • Dupuytren contracture (slides 28-31) • Hand fractures (32-45) • Hand palsy (46-57) • Sry, but I got the guidelines after finishing the seminar
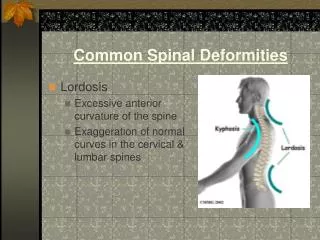
Hand Deformities • Mallet deformity • Trigger Finger • Boutonniere Deformity • Swan – Neck deformity • Dupuytren contracture
Mallet Finger • Aka: baseball finger • Deformity in which the fingertip is curled in and cannot straighten itself • Due to injury to extensor digitorium tendons at DIPJ
Mallet Finger/Causes Forced flexion of the finger when finger is extended: . Sport Injury: Finger struck by volleyball, basketball or baseball when it is in extension . Other common mechanisms of injury include forcefully tucking in a bedspread or slipcover or pushing off a sock with extended fingers.
Mallet Finger/Presentation • After DIPJ forced flexion: inability to actively extend the distal joint, intact full passive extension • Often injury is painless or nearly painless • Dorsum of joint may be slightly tender and swollen • Order X-ray to make sure there are no fractures
Despite active extension effort, the distal interphalangeal joint of the index finger rests in flexion, characteristic of a mallet finger
This x-ray depicts a large, dorsal-lip avulsion fracture from the distal phalanx, a bony mallet injury.
Mallet Finger/Managment • Mallet finger splint (6-10 weeks) • Surgery: • In case of volar sublaxation of distal phalanx or avulsion fracture • K-wire (Kirschner wire)
Anteroposterior radiographic view of finger after 4 weeks. The longitudinal K-wire is blocking the distal interphalangeal joint from flexion to protect the repair
Trigger Finger • Trigger finger is the popular name of stenosing tenosynovitis, a painful condition in which a finger or thumb locks when it is bent (flexed) or straightened (extended).
Trigger Tension • Due to narrowing of the sheath that surrounds the tendon in the affected finger, or a nodule forms on the tendon. • Trigger finger is often an overuse injury because of repetitive or frequent movement of the fingers (ex. hobbies as playing a musical instrument or crocheting) • Trigger finger may also result from trauma or accident • It is called trigger finger because when the finger unlocks, it pops back suddenly, as if releasing a trigger on a gun.
Trigger Tension • Clinical Picture: • Affected digits may become painful to straighten once bent • May make a soft crackling sound when moved. • It props back suddenly when straightened • Symptoms are usually worse in the morning and improve during the day • Treatment: • local steroid injections and splinting (weeks to months) • Surgery: cut the sheath that is restricting the tendon.
Introduction of the needle into the tendon sheath at 45° to the palm for injection treatment.
Boutonniere Deformity • Aka: Buttonhole Deformity • Hyperflexion at the PIP joint with hyperextension at the DIP • Passive extension of the PIP joint is easy.
Boutonniere Deformity • Flexion deformity of the PIP joint, due to interruption of the central slip of the extensor tendon: • The lateral bands separate • The head of the proximal phalanx pops through the gap like a finger through a button hole • The DIP joint is drawn into hyperextension. Central Slip Lateral Band
Boutonniere Deformity • The 3 main etiologies: • RA and other inflammatory arthritides (most often) • mechanical trauma • burns and infections • An X-ray should be done to detect avulsion fractures
Boutonniere Deformity • BD in patients with RA can be classified into 1 of the following 3 stages, which serve as a guide to the appropriate management: • Stage I (mild) is the earliest stage and is the result of PIP joint synovitis with mild extensor lag that still can be corrected passively. The metacarpophalangeal (MP) joint usually is normal, and the DIP may or may not be hyperextended. • Stage II (moderate) is characterized by 30-40° of flexion contracture at the PIP joint and hyperextension of the MP joint as a compensatory mechanism. The finger has increased functional loss. Early passive extension still is possible. With time, soft-tissue contractures develop, and passive extension becomes restricted. • Stage III (severe) begins when the PIP joint can no longer be extended passively. Radiographs demonstrate destruction of the joint surfaces
Boutonniere Deformity Treatment: • Splinting 4 weeks minimal (6 weeks preferable): • safety-pin splint (<40 degree) • Dynamic spring splints (> 40) • Surgery: When the deformity is the result of a dislocation of the PIP joint • Surgery carries a relatively high risk of FAILURE to achieve completely normal functioning extension mechanism of the finger.
Dynamic spring extension splint Bunnell Safety Pin Finger Splint
Swan-Neck deformity • -the PIP joint is hyper extended . DIP joint is flexed. • Cause: • Volar plate becomes weak -> hyperextension of PIPJ -> flextion of DIFJ • Due to injury or inflammation (RA)
Swan-Neck deformity • Swelling and pain due to inflammation from injury or disease (RA) • X-ray is done to evaluate the joints (RA) and look for fractures. • Treatment: • A boutonnière deformity caused by an extensor tendon injury can usually be corrected with a splint (Murphy Ring Splints) that keeps the middle joint fully extended for 6 weeks • When splinting is ineffective, surgery may be needed. MURPHY RING SPLINTS
Dupuytren contracture • Pathologic condition of the hand in which the fascia of the palm are shortened and thickened • Common in south europe
Dupuytren contracture • Dupuytren's contracture is more common among people with diabetes, alcoholism, or epilepsy • The disorder affects both hands in 50% of people • The disorder is occasionally associated with other disorders: • Garrod's pads: thickening of fibrous tissue above the knuckles • Penile fibromatosis: shrinking of fascia inside the penis that leads to deviated and painful erections • Plantar fibromatosis: nodules on the soles of the feet
Dupuytren contracture • Symptoms: • The first symptom is usually a tender nodule in the palm • Gradually, the fingers begin to curl. • Eventually, the curling worsens, and the hand can become arched (clawlike) • Treatment: • Surgery to correct contracted (clawed) fingers
Hand Fractures/Hx • Hand trauma, industrial • Hand dominance • Hand injured • Mechanism of injury: • Clean/dirty environment • Position of the hand • Thermal, electric or chemical injury • Wearing jewelry on finger, removed • In assault: • Hand open or fist clenched • Lacerations (tendon injury) • Contact with mouth, teeth • Years since last tetanus immunization (esp. in lacerations and abrasions)
Hand Fractures/ P/E • Hand examination: • Compare with uninjured • Signs of inflammation, abrasions, erosions • Abnormal position (esp. fingers): rotational deformity • Location of injury • Capillary refill • Neurology: radian, median and ulnar nerve
With fingers flexed at the metacarpophalangeal and proximal interphalangeal joints and extended at the distal interphalangeal joints, fingers should all point toward the scaphoid bone
Examination of the patient's hand with the fingers flexed may clearly reveal a rotational deformity
Hand Fractures • Imaging: • X-ray: AP, lateral and oblique view • MRI, CT, Bone scan seldom needed • ED care: • Pain management, reduction, splinting, referral • Primary concern is preservation of function • Except for distal phalanx fracture, all pts. Should be referred to a hand surgeon
Boxer’s Fracture • A break in one or more metacarpal bones, usually the fourth or the fifth, caused by punching a hard object. Such a fracture is often distal, angulated, and impacted • Finger shorten posteriorly Fourth and fifth metacarpal fractures, oblique view
Scaphoid Fracture • Epidemiology • common in young men; not common in children or in patients beyond middle age • Mechanism • FOOSH resulting most commonly in a transverse fracture through the waist (middle) of the scaphoid Scaphoid fracture in the middle third or waist
Scaphoid Fracture • Clinical Features: • pain on wrist movement • tenderness in scaphoid region (anatomical "snuff box") • usually undisplaced • Investigations: • x-ray (AP/lat/scaphoid views with wrist exended and ulnar deviation) • +/- bone scan and CT scan • Note: a fracture may not be radiologically evident up to 2 weeks after acute injury, so if a patient complains of wrist pain and has anatomical snuff box tenderness but a negative x-ray, treat them as if they have a scaphoid fracture and repeat x-ray 2 weeks later to rule out a fracture • Treatment: • Undisplaced: cast • Displaced = open (or percutaneous) screw fixation
Colles’ and Smith Fracture • Colles’ Fracture: • Due to FOOSH • > 40 yrs, female (esp. osteoperosis) • Fx fragment: upward-dorsal angulation (fork-like appearance) • Smith Fracture: • Aka: reverse Colles’ fracture • Falling on the back of a flexed hand • Fx fragment: volar (palmar) displacment
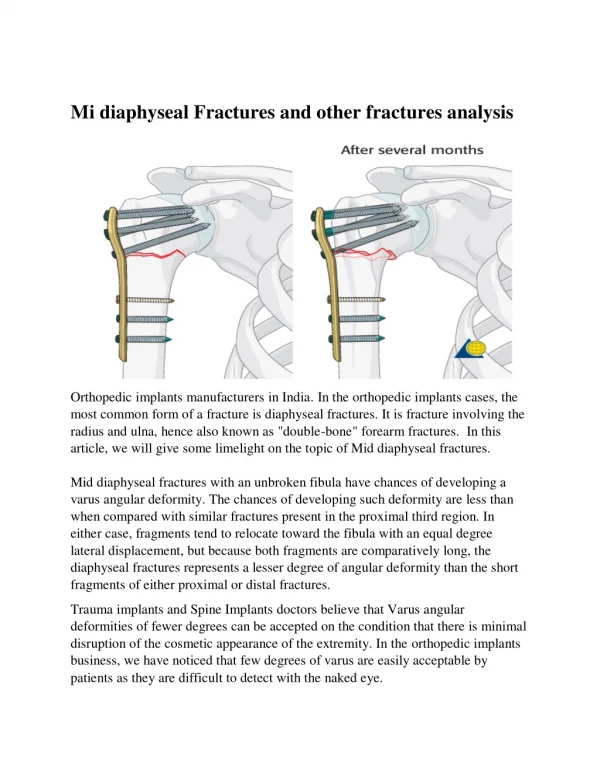
Both Bones Fracture (Radius & Ulna) • FOOSH, direct blow • Internal fixation by plates and screws • Complications: • Compartment syndrome • malunion Anteroposterior radiograph of a displaced, midshaft both-bone forearm fracture in an adolescent with a transitional growth plate
Ulnar nerve palsy • This occurs due to nerve compression at the elbow (cubital tunnel) or at the wrist (Guyon's canal) (Ulnar canal) • Muscle weakness and atrophy predominate the clinical presentation
Ulnar nerve palsy/Causes Cubital Tunnel Syndrome • Frequent bending of the elbow • Leaning on the elbow, resting it on an elbow, rest during a long distance drive or running machinery may cause repetitive pressure and irritation on the nerve. • A direct hit on the cubital tunnel may damage the ulnar nerve Guyon's Canal Syndrome • A cyst within the canal. • Clotting of the ulnar artery. • Fracture of the hamate bone. • Arthritis of the wrist bones
Ulnar nerve palsy/Causes • Symptoms & signs: • numbness and tingling in the ring and little finger and the sides and back of the hand. At Guyon's Canal, sensory supply to the skin of the back of the hand is spared. • The hand may become weaker resulting in trouble opening bottles or jars • Clawing may occur in the ring and little fingers • Froment's test: by asking the patient to hold a piece of paper between their thumb and index finger (hence checking adductor pollicis). In a patient with Ulnar nerve palsy the interphalangeal joint of the thumb will flex to compensate • Treatment: • Nonsurgical therapy: elbow or wrist splints to limit mobility in addition to an anti-inflammatory drug such as ibuprofen. • Surgical decompression maybe required in some cases