Download
1 / 48
480 likes | 530 Views
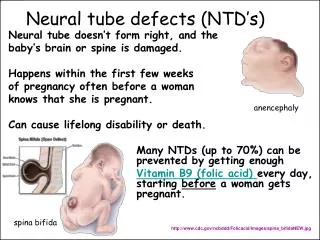
Learn about neural tube defects, spina bifida, hydrocephalus, and developmental dysplasia of the hip in children. Explore treatment options and signs to watch for.

E N D
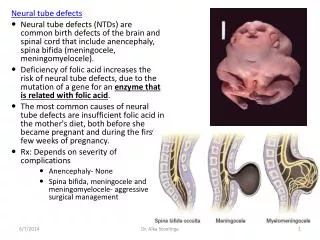
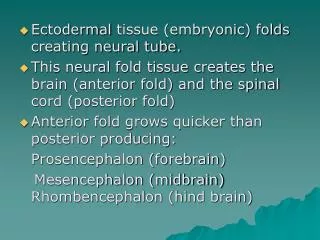
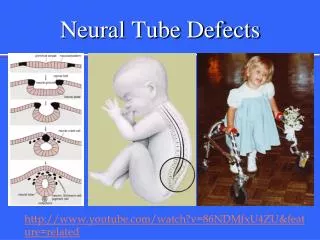
Neural tube defect • Encephalocele • Meningocele • Meylomeningocele
Encephaloceleبيرون زدگي مغز ومننژ از ميان نقص استخوان سر
Spina bifida • 1- Spina bifida(occulta) • 2-spina bifida cystica
Spina bifida نقص در تكامل تيغه خلفي ستون مهره ها • Occulta • Meningoceleبيرون زدگي پرده هاي مننژ • Meylomeningocele • بيرون زدگي پرده هاي مننژ همرا ه با شبكه نخاعي
Each shunt has 3 parts: • 1- Ventricular catheter: a small flexible tube which goes in the brain, in one of the cavities where the CSF is being retained. • 2- Reservoir : a small pump which regulates the amount of fluid that goes out. Through this the doctor can also check the working state of the shunt, as well as take CSF samples, when necessary, with a needle.
3- Distal catheter: another flexible tube that will take the fluid to the place where it is going to be absorbed. It is usually left with sufficient length, thinking in the child's growth.. • The shunts regulates the draining pressure. There are different levels of pressure, as high, medium and low. There are also some differences in the design but the means is always the same.
Developmental Dysplasia of the Hip(DDH) • Acetabular Dysplasia( preluxation) • Subluxation • Dislocation
Figure 3. A positive Galeazzi sign in a seven-month-old girl with left hip dislocation. Note the apparent femoral shortening
Figure 4. A three-year-old with a left hip dislocation. Note the limited abduction.
Figure 2. A 21-month-old child with right hip dislocation. Note the asymmetric skinfolds in the upper thigh
Figure 1. Tests commonly used to assess hip stability. (A) Ortolanimaneuver. A gentle upward force is applied while the hip is abducted. (B) Barlow maneuver. A gentle downward force is applied while the hip is adducted.
زمان تست • ارتولانی وبارلو = تولد تا 3-2 ماهگی بهترین زمان است • بعد از این سن (10-6 هفتگی)--->ایجاد انقباضات عضلات نزدیک کننده ران ---->محو علامت ارتولانی --
6 تا 18 ماهگی • کشش جا اندازی تدریجی (3هفته ) • پس از جااندازی 4-2 ما ه گچ اسپایکا
کودکان بزرگتر • مشکل است (تغییرات ثانویه در مفصل وفرم پا )(به طور کل بعد از 4 سالگی جااندازی سخت است ) • بعداز 6 سالگی غیر ممکن است • تنوتومی • استئوتومی • نوتوانی
Figure 7. A four-month-old child in a hip spica cast following bilateral closed reductions and adductor tenotomies
Figure 6. A newborn with bilateral hip dislocations in a Pavlik harness. The harness prevents hip extension and adduction but allows flexion and abduction