Download
1 / 74
830 likes | 1.55k Views
Hepatic Disorders: Hepatitis/Cirrhosis. Lisa Randall, RN, MSN, ACNS-BC RNSG 2432. Objectives. C ompare and contrast risk factors associated with hepatitis and cirrhosis Analyze the etiology and pathophysiology of hepatitis and cirrhosis

E N D
Hepatic Disorders:Hepatitis/Cirrhosis Lisa Randall, RN, MSN, ACNS-BC RNSG 2432
Objectives • Compare and contrast risk factors associated with hepatitis and cirrhosis • Analyze the etiology and pathophysiology of hepatitis and cirrhosis • Integrate diagnostic tests with etiology, pathophysiology, and signs/symptoms of both disorders • Formulate relevant prioritized nursing diagnoses that address physical, pyschosocial, and learning needs and evaluate nursing interventions
A Liver B Hepatic vein C Hepatic artery D Portal vein E Common bile duct F Stomach G Cystic duct H Gallbladder
Pathophysiology • Largest organ • Metabolic functions • Bile synthesis • Hepatocytes • Bile secretion • Storage • Mononuclear phagocyte system • Kupffer cells • Phagocytic activity
Metabolic functions • Metabolism of glucose • Protein • Fatty acids • Cholesterol
Other Functions • Immunologic • Blood storage • Plasma protein synthesis • Clotting • Storage of vitamins and minerals • Waste products of hemoglobin • Bile formation and secretion • Steroids and hormones • Ammonia • Drugs, ETOH, toxin metabolism
Pathophysiology • Inflammation • Hepatic cell necrosis • Proliferation/enlargement Kupffer cells • Cholestasis • Regeneration
Types • Chronic • Fulminant • Toxic • Hepatobillary
Hepatitis Types (Viral) • A • B • C • D • E • G *see handout
Clinical Manifestations Acute Chronic • Anorexia • N/V • RUQ pain • Bowel irregularity • Malaise • HA • Fever • Arthralgias • Uticaria • Weight loss • Jaundice • Hepatomegaly • Splenomegaly • Pruritus • Dark urine • Bilirubinuria • Light stools • Fatigue • Malaise • Easy fatigability • Hepatomegaly
Phases • Preicteric • Prodromal • Icteric • Jaundice • Posticteric • Convalescent
Hepatitis A • Fecal/oral • 15-50d • S/S • Light stools • Dark urine • Fatigue • Fever • Jaundice • Labs • Vaccine • IgG • Prevention
Hepatitis B • Percutaneous/permucosal • Sexual contact • Perinatal • 45-180d • S/S • 30% asymptomatic • Flu • Light stools • Dark urine • Fatigue • Fever • Jaundice • Labs • Prevention • Vaccine • IgG • Safe sex • No sharing of razors, toothbrushes, needles • Chronicity • Antivirals
Hepatitis C • Percutnaeous/mucosal • Sexual contact • Perinatal • 14-180d • S/S • 80% asymptomatic • HBV • http://youtu.be/y6osMO5xnag • Labs • Prevention • Safe sex • No sharing of razors, toothbrushes, needles • Chronicity • Interferon • antivirals
Hepatitis D • HBV • 2-26wk • Labs • Interferon • HBV vaccine • S/S • HBV
Hepatitis E • Fecal/oral • Contaminated water • Poor sanitation • 15-64d • Labs • S/S • HBV • No vaccine
Diagnostics • LFT • ALP • Serum bilirubin • Liver biopsy • Antigen specific
Treatment • Diet • High cal/protein, low fat • Vitamins (B, K) • ETOH/Drugs • Fluid management • Bed rest • Drug therapy • Prevention of HAV and HBV • Interferon • Lamivudine • Ribavirin • Acetaminophen
Nursing Diagnoses • Risk for infection (transmission) • Imbalanced nutrition • Disturbed body image • Knowledge deficit
Pathophysiology • Caused by destruction of liver cells, fibrosis and nodule formation restricting blood and bile flow • Normal hepatic blood pressure is near zero. Restriction of blood flow in liver dysfunction causes hypertension, and blood will attempt to find other pathways, bypass liver • Results in significant impairment of liver function • 80% destroyed before signs and symptoms • Liver can regenerate itself if good nutrition, rest, and no alcohol
Types of Cirrhosis Classified by risk factors • Post necrotic • Hepatitis • Alcoholic Cirrhosis • Laennec’s • metabolic changes in liver, particularly fat • Biliary • obstructive • Cardiac • right side heart failure • Drug induced • INH, rifampin, Tylenol
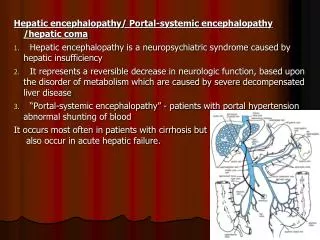
Signs & Symptoms • Liver enlarged • Dull pain RUQ • Weakness • Anorexia • Skin • Sclera • Portal hypertension • Splenomegaly • Ascites • Esophageal varices • Hepatic encephalopathy • Hepatorenal Syndrome • Liver failure
Jaundice • Excess bilirubin • Heptocellular • Cirrhosis • Obstructive • Hemolytic • Excessive destruction of RBCs • Transfusion reaction • Autoimmune • Faulty hemoglobin • Sickle cell
Diagnostics • LFT • CBC • Coags • Bilirubin • Albumin • Ammonia • Esophagascopy • Liver biopsy *See Table 44.15
Liver Biopsy • 3 types • Needle • Laparoscopic • Transvenous • Catheter • Blood clotting problems • Excess fluid • Complications • Puncture of lung or gallbladder • Infection • Bleeding • Pain
Liver Biopsy • Adequacy of clotting- PT/ INR, Platelets (Vit. K?) • Type and cross match for blood • Stop aspirin, ibuprofen, and anticoagulants 1 wk. before • Chest x-ray • Consent form & NPO 4 to 8 hr. • Vital signs & Empty bladder • Supine position, R arm above head • Hold breath after expiration when needle inserted • Be very still during procedure – 20 minutes
After Needle Liver Biopsy • Pressure • Right side • minimum of 2 hrs • flat 12-14 hrs • Vital signs & check for bleeding • NPO X 2 hr after • Assess for peritonitis, shock, & pneumothorax • Rt. shoulder pain common • caused by irritation of the diaphragm muscle • usually radiates to the shoulder a few hours or days. • Soreness at the incision site • Tylenol • avoid aspirin or ibuprofen for the first week because they decrease blood clotting, which is crucial for healing. • Avoid coughing, straining, lifting x 1-2 weeks
Nursing Assessment • LOC • Reflexes • Hyperreflexia • Pupils • Orientation • Sensory/motor • Asterexis • http://www.youtube.com/watch?v=pAOWjYo-sX4 • Coordination • Dysmetria • Fluid/electrolytes • Acid/base imbalances See table 44.17
Nursing care • Safe environment • Sustain life
Nursing Diagnoses Hepatitis Cirrhosis • Risk for infection (transmission) • Imbalanced nutrition • Disturbed body image • Knowledge deficit • Excess fluid volume • Disturbed thought process • Ineffective protection • Impaired skin integrity • Imbalanced nutrition • Knowledge deficit
Treatment • Diet • Sodium restriction • High carbs • Mod fat • 75-100gm protein • 60-80gm/d (hep encephalopathy) • Fluid management • Drug therapy • Diuretics • Laxatives • Anti-infective agents • Surgical/medical interventions
Major Complications of Cirrhosis Portal hypertension Variceal bleeding Ascites Spontaneous bacterial peritonitis Splenomegaly Hepatorenal syndrome Hepatic encephalopathy
Portal Hypertension • Arteriovenous shunting • Marked ascites • Caput medusae • Dilated abdominal veins • Esophageal varices • Hemorrhoids • Hyperslenism • Mod anemia • Neuropenia • Thrombocytopenia
Surgical/Medical Interventions • Paracentesis • Gastric lavage • Balloon tamponade • Schlerotherapy • Banding • TIPS (transjugular intrahepatic portosystemic shunt) • Liver transplant
Ascites • Sodium restriction • Bedrest initially • Diuretics • Spironolactone • Lasix • HCTZ • Fluid removal • Paracentesis • Peritoneovenous Shunt
Ascites Caput medusae
Paracentesis • Only used if respiratory distress • Pt will loose 10-30 grams of protein • Pt in sitting position • Empty bladder first • Post--watch for hypotension, bleeding, shock & infection
Esophageal varices • Collateral vessels • Complex of swollen, enlarged veins • Portal hypertension • 2/3-3/4 • Bleeding • LIFE-THREATENING