Download
1 / 26
310 likes | 1.81k Views
Fulminant Hepatic Failure- Acute Hepatitis B. AM Report 07/07/09 Amy Auerbach . Fulminant Hepatic Failure. Rapid development of severe acute liver injury with impaired synthetic function and encephalopathy In a patient who previously had a normal liver or had well-compensated disease.

E N D
Fulminant Hepatic Failure- Acute Hepatitis B AM Report 07/07/09 Amy Auerbach
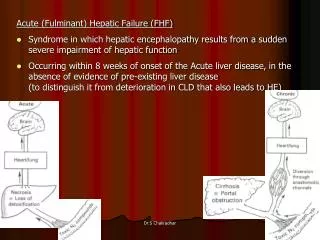
Fulminant Hepatic Failure • Rapid development of severe acute liver injury with impaired synthetic function and encephalopathy • In a patient who previously had a normal liver or had well-compensated disease
Etiology of Fulminant Hepatic Failure • Toxins: Most common cause- Acetaminophen is the most common toxin; augmentin second most likely toxin • Viral: Most common viral cause are the hepatitis viruses (hepatitis B more commonly progresses to FHF than hepatitis A) • EBV, CMV, HSV, Varicella also potential etiologies • Vascular: Portal vein thrombosis, Budd-Chiari syndrome, veno-occlusive disease, ischemic hepatitis • Metabolic: Wilson’s disease, acute fatty liver of pregnancy, Reye’s syndrome • Other: Autoimmune hepatitis, malignant infiltration of the liver, sepsis
Complications • Encephalopathy • Cerebral edema • Hypoglycemia • Metabolic acidosis • Sepsis • Coagulopathy • Multiorgan Failure
Treatment Acetaminophen toxicity: NAC (NAC now used in non-acetaminophen related cases of fulminant hepatic failure as well) Herpes: Acyclovir Autoimmune: Steroids Budd-Chiari- Heparin/TIPS Supportive Care: Lactulose, stress ulcer prophylaxis, FFP if actively bleeding, antibiotics for infections Transplantation in all etiologies EXCEPT for infiltrating cancer (breast, melanoma, lymphoma)
Hepatitis B Infection- Epidemiology • Perinatal transmission most common in high prevalence areas • Horizontal transmission (in early childhood) accounts for most cases in intermediate prevalence areas (minor breaks in skin or mucous membranes) • Unprotected sexual intercourse and IVDA in adults accounts for most of spread in low prevalence areas • Progression to chronic hepatitis B is much more common with perinatal transmission
Acute Hepatitis • 70% of patients with acute hepatitis B have subclinical or anicteric hepatitis • 30% develop icteric hepatitis • .5-1% develop fulminant hepatic failure: believed to be secondary to massive immune-mediated lysis of infected hepatocytes
Acute Hepatitis B • Incubation period lasts 1-4 months • May develop anorexia, jaundice, nausea, RUQ discomfort • Symptoms and jaundice typically resolve after 1-3 months • Lab testing reveals elevations in ALT and AST up to 1000-2000 IU/L
Outcome after Acute Hepatitis B • Traces of HBV often detectable in blood by PCR many years after clinical recovery • Persistent histologic abnormalities may be present many years after serologic recovery • Latent infection can maintain the T cell response for decades following clinical recovery
Hepatitis B Serologies • HBsAg: Hepatitis B surface antigen- appears 1-10 weeks after an acute exposure to HBV - Usually becomes undetectable after four to six months - Persistence of HBsAg for more than six months implies chronic infection • Anti-HBsAg- follows dissapearance of HBsAg - Typically persists for life and confers long term immunity - May not be detectable until after a window period of several weeks to months during
Hepatitis B Serologies • IgM anti-HBc: IgM antibodies against hepatitis B core antigen: allow serologic diagnosis to be made during the “window period” and can help differentiate between acute and chronic infection • Anti-HBc: hepatitis B core antigen- intracellular antigen expressed in infected hepatocytes: can help differentiate between immunized patients and patients who have cleared infection
Hepatitis B Serologies • HBeAg: Hepatitis B e antigen- secretory protein processed from the precore protein • Considered to be a marker of HBV replication and infectivity • HBeAg to anti-HBe seroconversion occurs early in patients with acute infection- prior to HBsAg to anti-HBs seroconversion
Typical levels of alanine aminotransferase (ALT), HBV DNA, hepatitis B s and e antigens (HBsAg and HBeAg), and anti-HBc, anti-HBe, and anti-HBs antibodies are shown in acute self-limited HBV infection (Panel A) and in infections that become chronic (Panel B). The intensity of the responses, as a function of time after infection, is indicated schematically. HBV DNA may persist for many years after the resolution of acute self-limited infection.42
Chronic Hepatitis B • May have stigmata of chronic liver disease: jaundice, splenomegaly, ascites, peripheral edema • Mild elevation in serum AST/ALT • Progression of cirrhosis is possible • Extrahepatic manifestations: polyarteritis nodosa and glomerular disease
Replicative Phase: Immune Tolerance and Clearance • High levels of HBV replication: presence of HBeAg and high levels of HBV DNA • No evidence of active liver disease • Immune tolerance usually lasts 10-30 years- in this time there is a very low rate of spontaneous HBeAg clearance • Immune clearance occurs during second and third decades in patients with perinatally acquired HBV infection
Inactive Carrier State • HBeAg negative and anti-Hbe positive • These patients can still have significant histologic inflammation and/or fibrosis
Complications of Chronic Hepatitis B • Cirrhosis • HCC: surveillance for HCC recommended for chronic HBV carriers • Reactivation following seroconversion: patients who receive immunosuppressive therapy (can also occur spontaneously) • Vaccinate against hepatitis A and caution re: alcohol, acetaminophen use
Treatment • Adult course is typically self-limiting • In fulminant hepatic failure, lamivudine most commonly used (L-nucleoside agent) • Patients with compensated cirrhosis and detectable level of HBV DNA are candidates to prevent progression • Threshold for treating HBeAg-positive chronic HBV infection is lower than for HBeAg negative infection
Back to our case… • Multiple reports of HBV reactivation in patients undergoing chemotherapy: risk is greatest upon withdrawal of treatment • Risk is greatest for patients who are: HBsAg positive, male gender, use of corticosteroids, use of rituximab • Other risk factors for reactivation: - HIV infection, superinfection with other hepatitis viruses, interferon therapy, corticosteroids, immunosuppressive therapy
Can reactivation be prevented? • Mutliple studies have suggested a benefit from prophylactic use of antiviral treatments in patients at risk for HBV reactivation • Anti-viral most commonly used is lamivudine • Started before chemotherapy and maintained at least six months after withdrawal of chemotherapy
Take Home Points • Acetaminophen toxicity is the most common cause of fulminant hepatic failure • Hepatitis B is the most common viral cause of fulminant hepatic failure • Anti-HepBc can help you tell the difference between an immunized patient and a patient who is “naturally” immune (positive in the patient who was exposed to infection) • IgM Anti-HBc is most useful during the “window period” • Prophylactic lamivudine can be used in setting of immunosuppression and chronic hepatitis B
References • Uptodate.com • Dienstag, Jules. Hepatitis B Virus Infection. NEJM Volm 359:1486-1500 • Lau GK et al. Early is superior to deferred preemptive lamivudine therapy for hepatitis B patients undergoing chemotherapy. Gastroenterology, 2003; 125:1742-1749