Equine Hepatic System: Disease & Abnormalities Overview
Learn about symptoms, diagnostics, and treatments of hepatic diseases in horses. Understanding key aspects for timely intervention.

Equine Hepatic System: Disease & Abnormalities Overview
E N D
Presentation Transcript
Abnormalities that occur with hepatic disease • Photosensitization (25%) • Hepatoencephalopathy (80%) • Coagulopathies • Icterus • Mild to moderate colic • Pruritis • Ascites is fairly infrequent • Weight loss (w/ chronic)
CBC • Mostly nonspecific changes • Evidence of hemolytic disease (red discoloration etc) • WBC and fibrinogen indicate inflammation
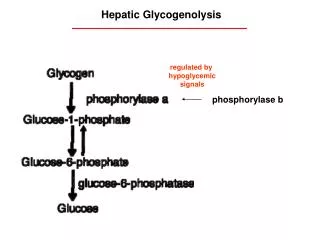
Chemical profile • Hypoglycemia • BUN • Low values indicate liver disease • Variable by lab and diet • Horses rarely have hypoproteinemia associated with liver disease • Increased bile acids • Sensitive indicator especially in chronic cases • Can do bile acids anytime (horses don’t have a gallbladder so there aren’t any pre or post prandial concerns)
Liver enzymes • SDH • Liver specific • Will increase due to even very mild hepatic trauma or in colic despite direct hepatic damage (acute) • ALP • Not liver specific • High levels in foal due to anabolism in skeleton • Associated with biliary system (acute) • AST (SGOT) • Not liver specific: mostly in hepatocytes • ½ life is longer so it indicates chronic dz • GGT • Fairly liver specific • Derived from biliary cells • Increases tend to persist for weeks (chronic dz)
Icterus • Evaluated through bilirubin levels • Unconjugated bilirubin • Calculated (Indirect) • Increased levels can be associated with anorexia • Conjugated bilirubin • Measured (Direct) • Ration of direct to total bilirubin > 25% is associated with cholestatic disease
Photosensitization • 25% of cases • 2 types of photosensitizing agents • Photoallergic • Phototoxic • Typically only white areas affected
Hepatic encephalopathy • 80% • CS: frequent yawning, behavioral change, generic CNS signs etc • Pathophysiology • Blood ammonia elevated (other toxins may act synergistically with ammonia) • Amino acids (decreased branched chain AA, increased aromatic amino acids) • Increased aromatic AA may lead to formation of increased inhibitory neurotramsitteres, alterations in catecholamines • Tx • Low protein diet and supplement with branch chained AA
IDIOPATHIC ACTIVE HEPATIC DISEASE • Aka Theilers disease, serum sickness • Mostly ADULTS • Most frequently associated with tetanus antitoxin but also associated with any equine serum product • Etiology • Increased incidence in certain geographic areas • Possible viral infection
IDIOPATHIC ACTIVE HEPATIC DISEASE • CS • Onset abrupt • Fever absent • W TAT onset begins 4-10 weeks post vaccination • General liver disease signs (hepatic encephalopathy, photosensitization etc) • Dx • Elevated bilirubin, AST, SDH, GGT • Necropsy: small flaccid liver, icteric carcass
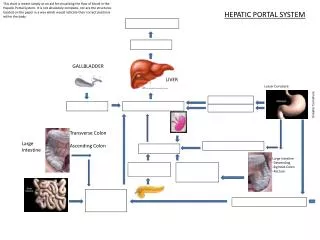
CHOLELITHIASIS • Choledocholelithiasis (common bile duct) is the most common biliary obstruction in the horse (occurs more frequently in the horse than in other domestic animals) • Pathogenesis • Unknown: ascending infection, parasites, foreign body etc) • Composition of stones: mixed • Bilirubin, CaPO4, cholesterol esters, bile pigments etc
CHOLELITHIASIS • Signalment: ADULTS, no breed or sex predilection • Risk factors: enteric Gram – infection from SI • CS • Intermittent abdominal pain w pyrexia and icterus • Less commonly HE, photosensitization, weight loss • Lab evaluation • Increased liver enzymes (GGT, ALP, bile acids) • Suspect cholestasis if direct is >30% of total bilirubin
CHOLELITHIASIS • US: definitive diagnosis • Hepatomegaly and bile duct dilation • Generally multiple choleliths seen • Tx • Medical: • long term broad spectrum AB’s (enrofloxacin/ ceftiofur) • Fluid therapy • DMSO: helps dissolve Ca glucoronidate calculi • Bile salt therapy: contraindicated in horses • Surgical: relief of obstruction • Guarded prognosis • Monitoring • Repeat US, sequential GGT/ALP
CHRONIC ACTIVE HEPATITIS • Eiology • Unknown (maybe toxins or bacteria from GIT) • CS • Progressive weight loss, intermittent fever and icterus • Some develop peculiar cutaneous lesions • Lab Evaluation • ALP, GGT, bile acids increased • Liver biopsy: cholangiohepatitis on histopath
CHRONIC ACTIVE HEPATITIS • Tx • Supportive care • Corticosteroids where lymphocytic-plasmacytic infiltrates • AB if bacterial infection • Prognosis • Based on liver biopsy and response to therapy • Poor if functional liver failure and fibrosis • Fair to good if early lesions
PYRROLIZIDINE ALKALOID TOXICITY • Risk factors • Ingestion of PA containing plants (dose cumulative) • Not usually very palatable • Pathophysiology • Antimitotic effect on DNA -> hepatocytes cannot divide -> die + replaced by fibrosis • CS • Chronic liver failure signs • Occasionally pruritis • Abortion
PYRROLIZIDINE ALKALOID TOXICITY • Lab evaluation • Liver enzymes elevated • Liver biopsy • Triad of fibrosis, bile duct proliferation, and megalocytes • Prognosis • End stage fibrosis = grave
TYZZERS DISEASE • Signalment: 7-40 days of age; FOALS • EA: Clostridium piliformis • Risk factors: parturition • Pathophysiology • Fecal-oral route of transmission • Carrier state may exist ???? • Not a highly contagious disease • CS • Often found dead w no history of signs • Fever, depression and anorexia • Icterus, hypoxia, coma, seizures etc
TYZZERS DISEASE • Dx • Lab evaluation • elevated enzymes, severe hypoglycemia • Definitive dx only at post mortem • Organism not readily id in routine stains • Tx • No reports of successful tx • Antimicrobial therapy (pen, tetracyclines, erythromycin)
HEPATIC FAILURE IN FOALS • CS • Hepatoencephalopthy w icterus • Some die peracutely • Etiology • Precolostral iron, perinatal herpes, lepto, tyzzers, duodenal ulcers, ascarid migration, hepatotoxicities • PSS infrequent • Dx • Increased bilirubin, ammonia and prolonged PT • SDH often normal; most foals normally have elevated GGT
GENERAL TREATMENT OF LIVER DISEASE • Agitation/convulsing: xylazine/ AVOID diazepam • Low glucose: give 10% glucose IV • Decrease blood ammonia • Oral lactulose, mineral oil/oral neomycin • Metronidazole • Correct acidosis • only if moderate to severe, correct very slowly or HE will worsen
GENERAL TREATMENT OF LIVER DISEASE • Decrease Hepatic workload • 5-10% dextrose drip • Dietary management • Small meals frequently • Force feed if not eating • Branched chain AA supplement • Bactericidal Abs • Ampicillin/gentamicin, TMS, ceftiofur
GENERAL PROGNOSIS IN LIVER DISEASE • Typically poor if • Low albumin levels • PT which is 30% longer than normal • Large increase in GGT/ ALP w normal or decreased SDH • Marked fibrosis that bridges liver lobules
PHEOCHROMOCYTOMA • Benign unilateral tumor of the adrenal medulla • Signalment: >12 years old • CS: excessive sweating, PU/PD, tachycardia, dilated pupils, hyperglycemia • Dx: difficult antemortem • Blood and urine levels of catecholamines • Tx • Surgical removal • Grave prognosis: often too ill to be treated
HYPOTHYROIDISM • Overdiagnosed dz • Clinical manifestations • Skinny, poor-doers, poor performance • Exertional rhabdomyolysis • CS • Decreased food intake • Dull hair coat, scaly, hypothermia, lethargic, thyroid enlargement • Dx • Baseline T3 and T4 • Do TRH or TSH stim to verify
HYPOTHYROIDISM • Tx • Supplementation: very controversial • Many report the absence of any response to thyroid supplements, some conditions are thyroid responsive w/o being hypothyroid
HYPERTHYROIDISM • There are no reported cases of equine hyperthyroidism
PIPD • Pars intermedia dysfunction • Signalment • Most common disease associated with advancing age • No sex predilection • Ponies more frequently affected than horses • Pathophysiology • Loss of dopaminergic control w/I Pars intermedia • Secretion of POMC by melanotrophs is regulated by inhibition via dopamine • Produce large amounts of alpha MSH and beta endorphins
PIPD • CS • Coat abnormalities (85%) Hairy • Chronic or recurrent laminitis (low grade) • 52% of cases (33% in geriatric population) • Sole abscesses are a major problem • PU/PD • Type 2 diabetes (38%) • Hyperhydrosis • Muscle wasting • Weight loss in very advanced cases
PIPD • Lab evaluation • CBC • typically normal (may have stress leukogram or mild anemia) • Chemistries • Hyperglycemia (33%), Hyperinsulinemia (62%), cortisol often normal, high ACTH • Special diagnostics • Cortisol (future gold standard) one sample in AM, second sample 8-10 hours later…in PIPD les than 30% variation • Dex suppression (gold standard) • Give dex and draw post samples at 5 different times • May worsen or cause laminitis
PIPD • Tx • Excellent management w exercise to maintain muscle tone • Cyproheptadine • Little evidence that the drug should be efficacious but it appears to be effective • Pergolide • Treatment of choice • Dopamine receptor agonist; decreases POMC • Clinical improvement expected in 6-8 weeks • Prognosis: predicted by the degree of hyperglycemia
HYPERLIPIDEMIA/ HYPERLIPEMIA • Hyperlipidemia: serum triglyceride is increased but less than 500 mg/dl • Hyperlipemia: serum triglyceride in excess of 500 mg/dl • Signalment: pony and pony crosses, mini horses, donkeys and mini donkeys • Risk factors • Obesity • Lactation/ pregnancy • Stress/ transportation • Can be a complication of any primary disease when a severe energy dietary imbalance occurs in high risk breed
HYPERLIPIDEMIA/ HYPERLIPEMIA • Pathophysiology • Negative energy balance results in FA mobilization from adipose tissue • Ketone pathway poorly developed in horses therefore TG’s get stuck in the blood • May exacerbate malaise and may prolong recovery from the primary disease • CS • CS of primary disease • Lethargy, ADR, depression and anorexia • CS often nonspecific
HYPERLIPIDEMIA/ HYPERLIPEMIA • Dx • Serum triglyceride levels • Evaluation of hepatic and renal function • Diagnosis of primary disease • Monitor serum to catch early (visualize serum) • Tx • Most important factor- nutritional support • Reverses negative energy balance • Try to get them to eat anything (give a variety and let them nibble each thing) • Glucose drip to aid in increasing appetite • Resolve the primary disease
HYPERLIPIDEMIA/ HYPERLIPEMIA • Tx • Heparin therapy • Used to be recommended but not much improvement with heparin b/c its not typically a problem with peripheral utilization of FFA • Contraindicated in individuals with impaired coagulation from decreased hepatic function (d/t fatty infiltration) • Insulin therapy • Blocks mobilization of adipose tissue • Increases peripheral uptake and use of TGs from the blood • Prognosis • Grave (mortality 43%) • Prognosis worse in cases of renal involvement rather than just hepatic involvement