Download
1 / 40
400 likes | 607 Views
A happy liver and guts. In flow HA PV/SMA itoh Out flow Hepatocyte Biliary tree Macrophage Metabolic activity Enterocytes Gut ischaemia. Assessment of Liver Function and splanchnic circulation.

E N D
A happy liver and guts In flow HA PV/SMA itoh Out flow Hepatocyte Biliary tree Macrophage Metabolic activity Enterocytes Gut ischaemia
Assessment of Liver Function and splanchnic circulation • The following have been utilised to assess liver function and splanchnic circulation • 1.Liver biochemistry and Lactate • 2. Galactose and Indocyanine Green • 3. Arterial ketone body ratio • 4. Gastric C02 gap • 5. MEGX
Aim : optimal liver function - -Monitor appropriately -Examine the effects of our interventions Alter ventilation and not review gases Alter drug therapies and not look at urine output or haemodynamic data We assume global = local Main problem has been lack of bed side applicability
Flow dependency in the splanchnic bedCreuter et al Am J Resp Crit Care Med 1999 160(3):839, De Baker et al Am Rev Resp Crit Care Med 1998 157(4 pt 1):1219 No relationship between C02 gap and HSBF/CI Patients with a ratio of < 20% demonstrate flow dependency in the splanchnic circulation. 10% difference in HV and mixed venous saturations predicts flow dependency in the splanchnic bed Metabolically active area in sepsis Adequacy cannot be predicted by global measures
Isolated perfused rat liver, E.Coli +/- L-NMMA • E.Coli resulted in x 2 increase in wbc adherence • E.Coli + L-NMMA x 3 increase in wbc adherence • and 33% reduction in SBF • Nishida Am J Physiol 1994 267;G1135
Manipulations in the splanchnic bed • Splanchnic OER is normal or increased in sepsis • Metabolic rate is increased in the liver in sepsis : increased V02, lactate uptake and glucose output • Wang et al Arch Surg 1991 126 219, Dahn et al Arch Surg 1990 125 44, Surgery 1995;117:52 1, Dahn et al Am J Physiol 1995, Surgery 1990, 1995, Roukonen Crit Care Med 1993, Rheinelt Anaesthesiol 1997 • Hepatic dysfunction may be predicted in a group of patients with increased hepatic inflammatory output Increased IAP leads to inflammation Poeze Shock 2002 17(6):451-8 Hsu J Trauma 2004 57(3):569 • Physiological interventions may effect splanchnic blood flow, hepatocyte function and energy dependant transporters • Pressor drugs, Anaesthetic agents • Volume loading, Venous pressure : HV outflow and impaired arterial inflow, surgical techniques, IAP • Intra-abdominal hypertension
Splanchnic perfusion • Laparoscopy (pigs) : Decreased ICG clearance with increases in IAP Blobner Anaesthesiology 1998, 89:475 • Effect of fluids not predictable Sakka et al B J Anaesth 2001 86(5):657 • Dobutamine : increase in spl D02 and CI, No change in glu turnover Ensinger et al Anaesthesiol 1999, Rheinhelt Anaesthesiology 1997:86:818 • Dopexamine : no effect separate to that on Cardiac output Keifer Am J RCCM 2000:161:775 • Adrenaline : variable spl D02, increased metabolism glu turnover Meier Hellman et al 1997 Crit care Med , Vincent CCM 2003 • Iloprost: increased spl D02, decreased glu production, NS increase in spV02 Keifer P Int Care Med 2001 27(7):1110 • Phenylephrine vs Noradrenaline • Decreased splanchnic blood flow, V02, lactate uptake and glucose production Reinelt Crit Care Med 1999,27:325
Barnes Am J Physiol 1985;248 R208 Increase IAP Decreased compliance Reduced flow in Coeliac A 42% SMA 61% Renal A 70% Increased FVP and decreased flow 65%
Operative decompression n=11 in face of oliguria / acidosis/IAP >25 mmHg • IAP fell 49±11 to 19±6.8 mmHg *** • Increased CI, RVEDV • Improved urine output and pHi • Chang J Trauma 1998 44(3):440 • Post liver transplant n=108, IAP > 25 mmHg X 2 • Observed in 32% of patients on day 1 and 2 post-op • Renal dysfunction 32 vs 8% RR with IAP >25 is 9.8% • Lower Pa02/Fi02 ratio pre extubation 164 vs 271 mmHg * • Slower extubation • Crtical value IAP 23-25 on ROC for renal and respiratory dysfunction • Biancofiore Trans Proc 2004 36; 547
Rats, IAP up to 30 cm H20 for 90’ then decompress then Bx at 30’ • In vivo GSH decreased in liver • Decreased hepatocyte survival on culture • Decreased in vitro GSH • Hsu J Trauma 2004 57(3):569 • 16 patients elective diagnostic laparoscopy • Reflectance spectroscopy in gastric mucosa at baseline , 8 and 12 mmHg • Gastric mucosal saturation 69±7 to 63±8 * to 54±13%** - returned to baseline at release of IAP • No change in any other parameter • Schwarte Anaesthesiology 2004 100(5):1081
Decreased gastric, duodenal, jejenal, colonic, peritoneal and hepatic saturations using laser doppler if IAP > 15 • Schilling et al J Am Coll Surgeons 1997 184:378 • Decreased PV flow when IAP >10 • Takagi Surg Endosc 1998 12;427 • Animal study Diebel J trauma 1992 33: 45 and 279, Caldwell J Surg Res 1987 43:14 , Bongard J Trauma 1995 35;519 • Normal CI and MAP with IAP 20 cmH20 • PVBF decreased by 65% HABF decreased 45% • Decreased mesenteric perfusion • Decreased gastric pHi is those with increased IAP • Gastric tonometry improved in 75% of those after decompression • Surgue World J surg 1996; 20;988 • Ivatury J Trauma 1998 44 ;1016
Anaesthetized pigs • Klopfenstein Am J Physiol 1998 275;H900 • Blood drawn on 2 occasions and reinstituted ± C02 insufflation to IAP 15 mmHg • MAP and CI not changed • Increase in IAP associated with increase in portal venous and hepatic venous pressures • Functional Budd Chiari • Decrease THBF and renal blood flow
Pastor et al CCM 2001 29:1017 : Co2 insufflation in a Hemorrhagic pig model Baseline C1,2, Hemorrage H1,2 Reconstitution Insufflation C3 HA increases, PV decreases :Buffer Subsequent further increase in PVF Risk of “small for size syndrome” developing with prolonged changes
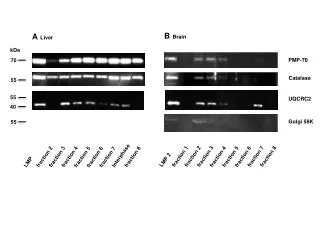
Pulse Densitometry Based on Pulse CICG mg/l 4 0 3 0 2 0 1 0 0 [ s ] 0 1 0 2 0 3 0 4 0 5 0 Measurement of ICG clearance from a finger probe ICG injected via peripheral or central vein LEDs 800 nm & 880 nm pulsatile800 nm non pulsatile800 nm pulsatile880 nm Sensor non pulsatile880 nm CICG = ratio of the pulsatile / non-pulsatile for both wave lengths Excellent correlation with arterial fibro-optic method r =0.96
Survival post hepatic resection IGC 5.2 ml/min/kg identified as cut off Hemming AW et al: Am J Surg 1992 ; 163 : 515 Correlation between parenchymal cell volume and ICG elimination Hashimoto M and Watanabe G: J Surg Res 2000 Wakabayashi W + Okochi J Surg Res 2004116(2):248 J Surg Res 2002 103(1) : Prognosis determined by ICG clearance +volume of liver resected in relation to native volume Hepatogastroenterology 46(27):1999: 1669 : liver resection 315 patients : 24 died ICG clearance and blood loss were predictors
Liver : supply and demand • 47 critically ill patients : 33 sepsis 16 non- septic • In the non septic group effective hepatic blood flow • and CO were correlated r=0.92 • Not seen in sepsis and EHBF/CO ratio was lower in NS than S • Surg Today 2003 33(2):101 • Loss of hepatic buffer response in sepsis Jakob et al Am J Physiol 2001;280:G819 • Hepatobiliary resections World J Surg 2002 26(4):457 • Hepatic ATP correlated with bile acid output and ICG excretion rate No correlation with bile flow
NAC and septic shock Rank et al Crit Care Med 2000 60 patients placebo vs NAC Increase in LBF (2.7 to 3.3) measured with ICG and CI (4.7 to 5.7) No change in LBFI/CI Increase in LV02 (85 to 103) and V02 Decrease in C02 gap (6.8 to 2.9) Increase in MEGX (16 vs -2) Improved energy charge on MRI spec Studies Spiers et al Crit Care2004
Survivors Non-survivors • Apache II 14 (10-18.6) 24 (18-25) ** • SAPS 40 (26 - 52) 62 (20-72) ** • Lactate 1.4 (1.1-2.2) 2 (1.5 - 4) ** • INR 1.4 (1.1-1.6) 1.53 (1.3-2.0) • Bilirubin 43 (17 - 93) 139 (54 - 194) ** • Pressors 7 / 44 15 / 35 ** • ICG 12.5 (8- 20.3) 5.5 (4.8 - 6.9)** • ROC and youden index were calculated for an ICG cut off of 9.65. • This results in a Sensitivity of 81%, Specificity of 73%, • Accuracy of 77%, PPV of 74% and NPV of 80% • IAP survivors 20(14-24) non-survivors 28(21-35) • Practical applications in following effects of fluid loading, pressor agents and effects of IAP
AUC for APACHE II 0.68, for SAPS II 0.755, ICG-PDR 0.745 Will there be any magic bullet ? Allows identification of an unhappy liver and monitoring of manipulations ICG clearance in sepsis Sakka et al Chest 2002; 122:1715-1720
Ent feed Spanchnic bed changes ALI PEEP • Post -operative patients - enteral feeding resulted in faster intestinal oxygen tension recovery Braga CCM 29 2001 • Cardiac surgery + vasoactive Rx post jejunal feeding resulted in increased ICG clearance Revelly Int Care Med 27 2001 • Post pyloric feeding in sepsis Enteral feeding associated with increase in HS blood flow, venous lactate:pyruvate ration stable, gastric C02 gap unchanged Rokyta Int Care Med 27 2001 Purcell 1993 : HS D02 and V02 in oleic acid dog model
donor and graft assessment Wesslau C et al: Transplantology 1994 ;5:1-3 PDR 15% cut off Jalan R et al: Transplantation 1994 ; 58 : 196-200 PDR 13.8 (10.8 - 21) vs 6.8 (5.7 - 14) p= 0.01 lactate 1.3 (0.9 - 2.8) vs 2.6 (1.6 - 4.6) p<0.01 in OLT patients Hepatobiliary: PDR 15.7 (12.2 - 24) vs 10 (5.5 - 14) p<0.01 Lactate 1.4 (1.1-1.85) vs 1.5 (1.3-1.5) NS
LiMon assessment in LITU • 79 patients were examined, median APACHE II score 17 (12-22), age 48 (20-70), 64 were ventilated and 21 were receiving noradrenaline. • 44 patients survived to ITU discharge and 35 died. • Data for the total group :- • MAP (mmHg) 79 (71-92) • CI (l/min2) 4.9 (4.1-6.1) • Lactate (mmol/l) 1.6 (1.2-2.4) • Albumin (mg/dl) 18 (13-24) • PDR (%/min) 9.4 (5.3-15) • Bilirubin (mmol/l) 84 (28-165)
25 20 15 10 5 0 Effect of NAC + PGI2 in sepsis Post OLT and ALF Devlin et al Int Care Med Useful in day to day care Post OLT + renal Tp Pancreatitis + sepsis “Well filled” Noradr 0.3 mcg/kg/min U/sound : high resistance flow++ ICG 9 Commenced NAC and PGI2 ICG 14 Post OLT ICG baseline 13 Developed Right heart failure RA26, PA 50/25 : ICG 8 Variety of therapies ICG 11 Track effects of pressor agents : particularly relevant with increased use of vasopressin
Where are we clinically ? • Monitoring standard tests….. Too late ?? • Lactate, LFT’s, Coagulation, Ultrasound, CT (MR) • Metabolism and flow • LiMon, COLD catheter MEGX, Hepatic vein sampling • Recognition of early liver dysfunction that has prognostic significance • Recognition of supply dependency within the splannchnic bed • More sensible application of vasoactive agents • Monitoring and thence avoidance of harmful manipulations and interventions • Search for the treatable endeavours to improve the liver
N=11 with ALI supine, prone (60’) then supine • No change in global haemodynamics • No change in IAP, HSBF or HSV02 or liver lactate uptake • Regional C02 unchanged • Matejovic et al Int Care Med 2002 28(120): 1750 • N=12 stable ALI prone : supine for 3 hours in random order • IAP 10±3 to 13 ±4 mmHg (NS) • CI, MAP : increased :3.8 to 4.4 L/min and 75 to 81 mmHg • PDR unchanged • Pa02/Fi02 increased (194±66 to 269±68) • Hering Int Care Med 2002 28(1):53
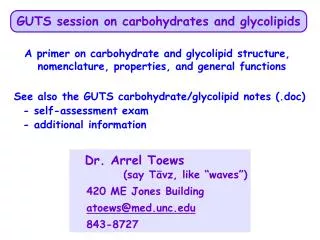
45 * 40 35 30 ICG-PDR [%/ min] * 25 (p< 0.001) 20 15 10 5 0 Survivors n= 168 Non-survivors n= 168 Significantly reduced liver function in non-survivorsSakka SG, Meier Hellmann A Yearbook of Intensive Care and Emergency Medicine, 2001 336 patients, lowest value for each individual correlated with poor outcome
ICG clearance in sepsis Sakka et al Chest 2002; 122:1715-1720 5.4 vs 14%/min 8.1 vs 14.7 %/min 11.9 vs 18.8 %/min
Composite measure of flow and hepatocyte uptake Nadir reached on day 7 178 patients studied on day of admission AUC for APACHE II 0.68, for SAPS II 0.755, ICG-PDR 0.745 Sakka SG et al chest 2002 122:1715-1720 AUC 0.745 0.755 0.688 Sakka et al Chest 2002; 122:1715-1720
Organ failures Bilirubin > 100µmol/L Pao2/Fio2 ratio< 200 Norepi/ epi >0.1µg/kg/min or dopamine >5 µg/kg/min Creatinine >300 µmol/L: < 500 ml urine/day GCS < 9 platelets < 100 Outcome of CLD in ITUWehler et al Hepatology 2001;34:255-261 143 patients :observational study, score at 24 hrs
Liver and sepsis • Hepatic metabolic response • HBF and hepatic V02 increased • Increased glucose output (76%), lactate uptake (5.3 to 16.4 µmol/min/kg), amino acid and alanine uptake were similarly increased. • Wang et al Arch Surg 1991 126 219 • Dahn et al Arch Surg 1990 125 44, Surgery 1995;117:520 • Roukonen Crit Care Med 1993, Rheinelt Anaesthesiol 1997 • Changes in splanchnic input and or metabolic changes are of great potential clinical significance • Dynamic microcirculatory changes in hyperdynamic sepsis • Decreased liver and pancreatic blood flow • Hilerbrand et al Crit Care Med 2000
Indications for liver transplantation Paracetamol Non-Paracetamol • pH < 7.30 pH<7.3 • all 3 of the following INR > 6.5 • within 24 hrs • PT > 100 INR > 6.5 any 3 of : • Creatinine > 300 µmol/l seronegative hepatitis or • grade 3 - 4 encephalopathy drug related / halothane • Bilirubin > 300 µmol/l • INR > 3.5 • Age < 10 yrs or > 40 yrs • J - E > 7 days Low P04 Lactate : 4 hrs > 3.5 OR 43 p<0.001 Lactate : 12 hrs > 3.5 OR 63 p<0.001 Children - coagulopathy INR > 4.5 Encephalopathy + Factor V < 20% or Budd Chiari : renal failure + HE < 30% if > 30 yrs of age
Lactate and galactose • Lactate level, regardless of source, appears to be a reliable prognostic indicator • Vincent Crit Care Med 1983, Bakker Am J Surg 1996,Record Metabolism 1981, De Backer Crit Care Med 1991, Friedman Crit Care Med 1995, Kellum et al Chest 1997 111:1301, Murphy et al Crit Care Med 2001;29:2111-2118 • Speed of response • Lactate load • Galactose and ICG • HV catheterization allows separation of extraction and flow • Multiple sampling • Research tool : not applicable at the bed side
40 y = 0,99x + 0,86 35 r = 0,96 30 25 PDR LiMON [%/min] 20 15 10 5 0 0 10 20 30 40 PDR COLD System [%/min] Invasive COLD System vs non-invasive LiMON(16 pts, n=54) Sakka Int Care Med 2000: 26; 1553
Anaesthetized pigs Klopfenstein Am J Physiol 1998 275;H900 • Blood drawn on 2 occasions and reinstituted ± C02 insufflation to IAP 15 mmHg • MAP and CI not changed • Increase in IAP associated with increase in portal venous and hepatic venous pressures • Decrease HBF and renal blood flow
Decreased gastric, duodenal, jejenal, colonic, peritoneal and hepatic saturations using laser doppler if IAP > 15 • Schilling et al J Am Coll Surgeons 1997 184:378 • Decreased PV flow when IAP >10 • Takagi Surg Endosc 1998 12;427 • Animal study Diebel J trauma 1992 33: 45 and 279, Caldwell `j `surg `res 1987 43:14 , Bongard J Trauma 1995 35;519 • Normal CI and MAP with IAP 20 cmH20 • PVBF decreased by 65% HABF decreased 45% • Decreased mesenteric perfusion
Pastor et al CCM 2001 29:1017 : Co2 insufflation in a Hemorrhagic pig model Baseline C1,2, Hemorrage H1,2 Reinstitution Insufflation C3
Abnormal liver blood tests • Normal liver blood tests can be seen in cirrhosis • Abnormal liver blood tests are a late feature and reflect established damage - not responsive enough to relate to acute changes • Elevated Bilirubin • Conjugated or unconjugated • AST / ALT • Hepatocyte damage • Lactate : composite measure of production and metabolic capacity - slow response time • GGT and Alkaline P04 • Drugs, alcohol, biliary disease - intra and extra hepatic • Sepsis and infiltration • Low AlkP04 in wilsons disease • INR and APTR • Useful in ALF as prognostic marker
Global splanchnic blood flow increased Increased flow with dopamine - no increase in Sp.V02 Clemmesen et al 1998 Hepatology Microcirculatory flow in animal model of sepsis: SMA flow restored after fluids but microcirculatory in pancreas, liver, colon and stomach remain significantly impaired Impaired stomach , pancreatic flow in rat model of ALF Increased C02 gap in ALF 0.5 to 3.5 at day 3 to day 6 post o/d Hitlebrand et al Crit Care Med 2000 Makin et al Am J Physiol 1996 Rhodes et al Int Care Med 2000
Hepatocyte and cannalicular transporters Splanchnic blood flow Uptake into hepatocytes Na+ independent organic anion transporting proteins (OATPs) Excretion into bile (MRP2) No entero-hepatic circulation ICG : Normal values ; . 700 mL/min/m2 and 18%/min Inert compound : taken up without metabolism Separate splanchnic blood flow and hepatocyte uptake utilising hepatic vein samples to calculate extraction