Fore word
Dear Doctor, This ECG presentation is an attempt to illustrate some of the fundamentals in ECG interpretation. We have advanced level courses also on ECG. In addition, we have several educational resource materials in the form of PowerPoint based CD-Rom

Fore word
E N D
Presentation Transcript
Dear Doctor, This ECG presentation is an attempt to illustrate some of the fundamentals in ECG interpretation. We have advanced level courses also on ECG. In addition, we have several educational resource materials in the form of PowerPoint based CD-Rom presentations. Also are available several philosophical and religious works of all time great masters, translated into simple English and presented as PowerPoint slide shows on CD-Rom. A list of such materials is appended. Pl. request for your copy of any of them at a nominal cost of Rs.100/ per CD. Wishing You a happy learning experience !! Fore word
The Objectives • To sensitize doctors towards learning ECG • To explain the clinical concepts involved • To illustrate them with diagrams, drawings, tables • To show real life ECG charts and interpret • Differential diagnosis on similar looking ECG changes • Spot light on ECG and Ischemic Heart Disease Not Included are • Electrophysiological basis of ECG changes • Details on arrhythmias, conduction disorders • Sensitivity and specificity of different patterns • Atypical presentations, combination of pathologies • Scoring systems and predictive values
Alan Lindsay’s Cyber ECG learning center (on line) Interactive Electrocardiography by Novartis – CD Rom Frank H Netter's medical drawings American Heart Association (AHA) sites American Heart Lung and Blood Institute (AHLBI) sites J.G. Webster’s Cyber ECG library Braunwald’s text book of cardiology - 6 ed. 2004 Goldberger’s text book on ECG Our personal collection of interesting ECGs ECG Resources consulted
ECG Graph Paper Y- Axis Amplitude in mill volts X- Axis time in seconds
X-Axis represents time - Scale X-Axis – 1 mm = 0.04 sec Y-Axis represents voltage - Scale Y-Axis – 1 mm = 0.1 mV One big square on X-Axis = 0.2 sec (big box) Two big squares on Y-Axis = 1 milli volt (mV) Each small square is 0.04 sec (1 mm in size) Each big square on the ECG represents 5 small squares = 0.04 x 5 = 0.2 seconds 5 such big squares = 0.2 x 5 = 1sec = 25 mm One second is 25 mm or 5 big squares One minute is 5 x 60 = 300 big squares ECG Graph Paper
ECG Complex P wave PR Interval QRS complex ST segment T Wave QT Interval RR Interval
ECG Complex • P Wave is Atrial contraction – Normal 0.12 sec • PR interval is from the beginning of P wave to the beginning of QRS – Normal up to 0.2 sec • QRS is Ventricular contraction –Normal 0.08 sec • ST segment – Normal Isoelectic (electric silence) • QT Interval – From the beginning of QRS to the end of T wave – Normal – 0.40 sec • RR Interval – One Cardiac cycle 0.80 sec
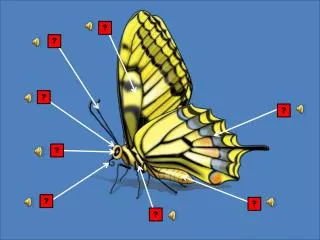
Identify the ECG Complex 3 4 5 1 8 2 6 7
Identify the ECG Complex The Wave or Interval Duration # of Boxes • P wave : Atrial contraction 0.12 sec (3) • PR interval – P to begin. of QRS 0.20 sec (5) • QRS complex - Ventricular 0.08 sec (2) • ST segment - Electrical silence Isoelectric • T wave - repolarization 0.12 sec (3) • QRS interval – Ventricular cont. 0.08 sec (2) • QT interval - From Q to T end 0.40 sec (10) • TP segment - Electrical silence 0.20 sec (5)
Let us Identify the waves 4 7 1 8 6 2 3 5
Let us Identify the waves • P wave – Atrial contraction = 0.12 sec (3 small boxes) • PR Interval – P + AV delay = 0.20 sec (5 small boxes) • Q wave – Septal = < 3 mm, < 0.04 sec (1 small box) • R wave – Ventricular contraction < 15 mm • S wave – complimentary to R < 15 mm • ST segment – Isoelectric – decides our fate • T wave – ventricular repolarization – friend of ST • TP segment – ventricular relaxation – shortened in tachycardia
Important Precautions • Correct Lead placement and good contact • Proper earth connection, avoid other gadgets • Deep inspiration record of L3, aVF • Compare serial ECGs if available • Relate the changes to Age, Sex, Clinical history • Consider the co-morbidities that may effect ECG • Make a xerox copy of the record for future use • Interpret systematically to avoid errors
Normal ECG • Standardization – 10 mm (2 boxes) = 1 mV • Double and half standardization if required • Sinus Rhythm – Each P followed by QRS, R-R constant • P waves – always examine for in L2, V1, L1 • QRS positive in L1, L2, L3, aVF and aVL. – Neg in aVR • QRS is < 0.08 narrow, Q in V5, V6 < 0.04, < 3 mm • R wave progression from V1 to V6, QT interval < 0.4 • Axis normal – L1, L3, and aVF all will be positive • ST Isoelectric, T waves ↑, Normal T↓ in aVR,V1, V2
Pediatric ECG • This is the ECG of a 6 year old child • Heart rate is 100 – Normal for the age • See V1 + V5 R >> 35 – Not LVH – Normal • T↓ in V1, V2, V3 – Normal in child • Base line disturbances in V5, V6 – due to movement by child
Normal Resting ECG – cannot exclude disease Ischemia may be covert – supply / demand equation Changes of MI take some time to develop in ECG Mild Ventricular hypertrophy - not detectable in ECG Some of the ECG abnormalities are non specific Single ECG cannot give progress – Need serial ECGs ECG changes not always correlate with Angio results Paroxysmal events will be missed in single ECG Be aware of normal ECG
Normal Variations in ECG • May have slight left axis due to rotation of heart • May have high voltage QRS – simulating LVH • Mild slurring of QRS but duration < 0.09 • J point depression, early repolarization • T inversions in V2, V3 and V4 – Juvenile T ↓ • Similarly in women also T↓ • Low voltages in obese women and men • Non cardiac causes of ECG changes may occur
Early Repolarization This ECG has all normal features The ST-T (J) Junction point is elevated. T waves are tall, May be inverted in LIII, The ST segment initial portion is concave. This does not signify Ischemia
Pseudo Normalization T↓ Before Chest pain T↑ During Chest pain T↓ Chest pain Relieved
Rate Determination QRS Next QRS
Rate Determination T ACHY NORMA L BRADY
What is the Heart Rate ? Answer on next slide
What is the Heart Rate ? • To find out the heart rate we need to know • The R-R interval in terms of # of big squares • If the R-R intervals are constant • In this ECG the R-R intervals are constant • R-R are approximately 3 big squares apart • So the heart rate is 300 ÷ 3 = 100
What is the Heart Rate ? Answer on next slide
What is the Heart Rate ? • To find out the heart rate we need to know • The R-R interval in terms of # of big squares • If the R-R intervals are constant • In this ECG the R-R intervals are constant • R-R are approximately 4.5 big squares apart • So the heart rate is 300 ÷ 4.5 = 67
What is the Heart Rate ? Answer on next slide
What is the Heart Rate ? • To find out the heart rate we need to know • The R-R interval in terms of # of Big Squares • If the R-R intervals are constant • In this ECG the R-R intervals are not constant • R-R are varying from 2 boxes to 3 boxes • It is an irregular rhythm –Sinus arrhythmia • Heart rate is 300 ÷ 2 to 3 = 150 to 100 approx
ECG Bipolar Limb Leads - + - - L R L R F + + F
ECG Bipolar Limb Leads • Standard ECG is recorded in 12 leads • Six Limb leads – L1, L2, L3, aVR, aVL, aVF • Six Chest Leads – V1 V2 V3 V4 V5 and V6 • L1, L2 and L3 are called bipolar leads • L1 between LA and RA • L2 between LF and RA • L3 between LF and LA
ECG Unipolar Limb Leads + + R L + F Lead aVR Lead aVL Lead aVF
ECG Unipolar Limb Leads • Standard ECG is recorded in 12 leads • Six Limb leads – L1, L2, L3, aVR, aVL, aVF • Six Chest Leads – V1 V2 V3 V4 V5 and V6 • aVR, aVL, aVF are called unipolar leads • aVR – from Right Arm Positive • aVL – from Left Arm Positive • aVF – from Left Foot Positive
ECG Chest Leads Precardial (chest) Lead Position • V1 Fourth ICS, right sternal border • V2 Fourth ICS, left sternal border • V3 Equidistant between V2 and V4 • V4 Fifth ICS, left Mid clavicular Line • V5 Fifth ICS Left anterior axillary line • V6 Fifth ICS Left mid axillary line
APC APC APC APC Atrial Ectopics
Atrial Ectopics • Note the premature (ectopic) beats marked as • APC (Atrial Premature Contractions) • These occurred before the next expected QRS complex (premature) • Each APC has a P wave preceding the QRS of that beat – So impulse has originated in the atria • The QRS duration is normal < 0.08, not wide
Atrial Fibrillation • Note ECG changes of Atrial Fibrillation • The heart rate is irregularly irregular • The R-R intervals are very different from beat to beat • There is narrow QRS tachycardia • There are no P waves – instead small fibrillary waves called ‘ f ’ waves are seen
Atrial Flutter Heart rate Rhythm P wave PR interval QRS in sec
Atrial Flutter • Note ECG changes of Atrial Flutter • The heart rate is regular or variable • Atrial rate is 300 per minute • All P waves are not conducted to ventricles • The R-R intervals very depending on the AV conduction ratio • The QRS is narrow – < 0.12 sec • The P waves have a ‘saw toothed’ appearance called ‘F’ waves
VPC VPC VPC VPC Ventricular Ectopics
Ventricular Ectopics • Note the premature (ectopic) beats marked as VPC (Ventricular Premature Contractions) • These occurred before the next expected QRS complex (premature) • Each VPC has no definite P wave preceding the QRS of that beat – So impulse has originated in the ventricles • The QRS complexes are wide with abnormal duration of > 0.12 and their shapes are bizarre
Ventricular Tachycardia • A wide QRS tachycardia is VT until proved • otherwise. Features suggesting VT include • Evidence of AV dissociation • Independent P waves (shown by arrows here) • Beat to beat variability of the QRS morphology • Very wide complexes (> 0.14 ms) • The QRS is similar to that in ventricular ectopics • Concordance (chest leads all positive or negative)
The Six Limb Leads FRONTAL PLANE RIGHT LEFT INFERIOR
The 12 Camera Photography • There SIX cameras photographing frontal plane • Lead 1 and aVL are horizontal left sided cameras • Lead 2, aVF, Lead 3 are vertical inferior cameras • aVR is horizontal Rt. sided camera (cavitary lead) • Lateral Leads – L1, aVL, V5 and V6 • Inferior Leads – L2, aVF, and L3 leads • Septal Leads – V1 and V2 • Anterior Leads – V3 and V4 • Anterio-lateral leads – V3, V4, V5, V6, L1 and aVL
The Six Chest Leads TRANSVERSE PLANE
The 12 Camera Photography • There SIX cameras photographing in transverse or anterio-posterior plane • V1 and V2 record events of septum • V3 and V4 record events of the anterior wall • V5 and V6 record events of left lateral wall • To record right side events V2R to V6R are needed – In dextrocardia, in RV infarction