Download
1 / 15
150 likes | 289 Views
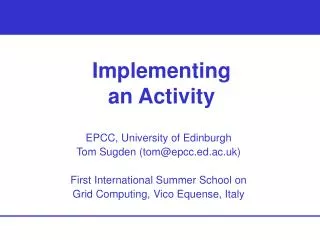
The Management of Neuroendocrine Tumours (NET) in Merseyside and Cheshire. An Audit of Activity and Pathways. Jon Hayes, Ged Corcoran and Chris Holcombe Sept 2008. DGH. Endocrinology. Gen Medicine. Surgery. NET Service. NET Clinician. NET Clinician. NET Clinician. NET Clinician.

E N D
The Management ofNeuroendocrine Tumours (NET) in Merseyside and Cheshire An Audit of Activity and Pathways Jon Hayes, Ged Corcoran and Chris Holcombe Sept 2008
DGH Endocrinology Gen Medicine Surgery NET Service NET Clinician NET Clinician NET Clinician NET Clinician NET MDT Further Investigations Therapy Biochem / Haematology Surgery Medical Treatment Radiology Imaging Interventional Radiology Radionuclide Therapy I131 MIBG or Y90 Dotatate Radionuclide Imaging Chemotherapy (DXRT) Immediate Post-Treatment Follow-up NET Service or DGH Long Term Follow-up and Surveillance
Merseyside and Cheshire NET Service The NET Service is provided by a number of local clinicians who have developed a special interest in this rare but complex condition. Incidence is around 2 per 100,000, but five year survival is around 70% so prevalence is high. Most patients require life-long follow-up and surveillance. Because the service has developed gradually over several years, only an informal clinical pathway has existed up until now. Consequently, important aspects of the service are not adequately funded. Some aspects of the clinical management are funded through PbR, but significant elements should be considered for collective and/or specialised commissioning. Neuroendocrine tumours have not been subject to NICE Improving Outcomes Guidance.
Diagnosis and Onward Referral NETs are usually diagnosed after investigation for non-specific symptoms (eg nausea, vomiting and diarrhoea) by physicians and surgeons in hospitals across the cancer network. Most carcinoid tumours arise in the appendix or small bowel. 269 out of 396 patients on the local NET database have carcinoid tumours (68%). Insulinomas, gastrinomas, phaeochromocytomas, glucogonomas, VIPomas and somatostatinomas account for the remaining 32%. NETs are associated with genetic syndromes such as Multiple Endocrine Neoplasia (MEN1 and 2), but most are sporadic isolated tumours. At the time of onward referral to the NET Service, many patients may already have had a laparotomy or biopsy to confirm the diagnosis.
Referrals Jan 2006 – end May 2008 (29 months): New patients = 162 (67 per year) Known deaths = 66 (27 per year) Site of primary: Source: NET database, Jan 2006 – May 2008.
Metastatic Disease Site of metastases: 53% of patients have metastatic disease. Source: NET database, Jan 2006 – May 2008. Total exceeds 100% as some patients have multiple sites recorded.
Assessment by NET Clinicians Referrals are made from DGHs to several clinicians with a special interest in NETs at the Royal Liverpool University Hospital and University Hospital Aintree. Referrals are received from trusts within the Merseyside and Cheshire Cancer Network, North Wales and the Isle of Man. Less frequent referrals are received from Lancashire, South Cumbria, Manchester and the rest of Britain. Patients are seen by the specialist clinicians in their outpatient clinics and then their cases are discussed at the NET Multidisciplinary Team Meeting (MDT). The NET MDT has developed in a gradual manner over several years and has met fortnightly since 2007. The meeting is chaired by Professor Vinjamuri, Consultant in Nuclear Medicine. The MDT has not had the benefit of an Oncologist (medical/clinical) for two years. It is likely that the MDT may need to be held weekly in the near future.
Additional Investigations Once referred into the NET Service, patients may require further diagnostic tests to assess the nature and extent of their disease. Biochemestry / Haematology • Full blood and urine endocrine profile - FBC • Renal function - Hepatic Function Imaging • Chest X-Ray • Contrast enhanced CT chest and abdomen • MR Radionuclide Imaging • I123 MIBG +/- Single Photon Emission Computed Tomography • In111 Octreotide +/- SPECT
Radionuclide Imaging Source: Peer Review Document, Dept of Nuclear Medicine, RLBUHT, 30 June 2008
Specialist Non-Surgical Therapies Hormone Therapy • Somatostatin analogues (12% of patients) • Patients receive monthly injections in the community co-ordinated by NET CNSs Chemotherapy (2%) • Co-ordinated by the most appropriate oncology centre for the patient (CCO, Christie, Glan Clwyd, Preston) Interventional Radiology • Radio-Frequency Ablation (1%) • Chemo-Embolisation (<1%) Radionuclide Therapies • I131 MIBG (5%) • Y90 Dotatate (8%) Figures in parentheses show proportion of patients (referred between Jan 2006 and May 2008) receiving these treatments recorded on the NET database.
Surgery 52% of patients have surgery. Location: Source: NET database, Jan 2006 – May 2008.
Radionuclide Therapies Source: Peer Review Document, Dept of Nuclear Medicine, RLBUHT, 30 June 2008
Post-Treatment Follow-up Patients are seen by the responsible clinician in outpatient clinics at the Royal and Aintree. On-going surveillance and management of recurrence Recurrence is common in this group of patients and follow-up continues for a number of years. Some patients are returned to their original referring network for surveillance. More locally, patients receive at least annual checks by NET clinicians.
For Discussion • Peer review measures stipulate minimum attendance at 50% of meetings for core MDT members. • Lack of CCO input to MDT needs to be addressed. • What investigations and treatments can be undertaken by referring hospital? • Trials recruitment: Is it as comprehensive as we would like? • What are the indications for specialist investigations and therapies? • Need to clarify which parts of the pathway are funded and how. Need to prepare a case for collective/specialised commissioners to consider regarding the unfunded elements. • What is the scope for developing the service beyond its current boundaries? • What is the role of PET-CT in NETs?