Download
1 / 40
400 likes | 526 Views
Welcome to the Neighborhood: Building A Medical Home for Alzheimer’s Disease. Soo Borson, MD Professor, Psychiatry and Behavioral Sciences Director, Memory Disorders Clinic and Dementia Health Services Research Group University of Washington. Dementia Health Services Research Group.

E N D
Welcome to the Neighborhood:Building A Medical Home for Alzheimer’s Disease Soo Borson, MD Professor, Psychiatry and Behavioral Sciences Director, Memory Disorders Clinic and Dementia Health Services Research Group University of Washington Dementia Health Services Research Group University of Washington
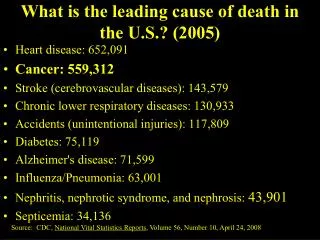
The Population Imperative Hebert et al. Neurology 2004
Framework: Caring Systems • Patients • Families • Providers • Internal medicine/ primary care • Specialty care • Social care • Health systems • Payers • Practice organizations © 3-11 Soo Borson MD
http://www.americangeriatrics.org/adgap/ADGAP; Brookmeyer et al, Am J Pub Health 1998 © 3-11 Soo Borson MD
A Primary Care Report Card *< 50% of specialists routinely disclose diagnosis (Raicher et al, Int Psychogeriatrics 2007). ** Wenger et al, Ann Intern Med 2003; Chodosh et al, JAGS 2007; Borson et al, JGIM 2007. ***Overall estimate based on studies of referrals to specialists, community resources, Alzheimer’s Association, explicit inclusion of caregivers as partners © 3-11 Soo Borson MD
Goals for Redesigning Primary Dementia Care • Detect cognitive impairment and diagnose dementia when it is present • Eliminate ‘don’t ask, don’t tell’ • Implement chronic care management model • Dementia is… • A medical problem caused by specific disease processes • A target for medical treatment • A risk factor for other problems • A (usually) progressive condition with changing, stage-specific management needs • A major determinant of the context of care
Rationale for Redesign– Clinical Improvement • Intervening early improves clinical outcomes for patients and families1 • Medical treatment • Donepezil for AD (multiple studies); other cholinesterase inhibitors • Psychological/behavioral interventions • Social and environmental approaches • Late detection delays secondary and tertiary prevention • Earlier detection of dementia makes sense 1 Feil et al for ACOVE team. JAGS 2007.
Rationale for Redesign – Health and Safety Systems • Health care • Delirium in hospital (OR 3.96, 95% CI 1.1-14.2) 1 • Low health literacy/adherence to pre-op instructions (OR 4.0, 95% CI 1.6-9.8) 2 • Deficit in knowledge/management of personal medications3 • Increased hospitalizations for ambulatory care sensitive conditions (OR 1.8, p < 0.0001) 4 • Public safety • Driving risk 5 • At home, in the community • Need for everyday support and assistance 6 • Alagiakrishnan et al. JAGS 2007. 2. Chew et al. Am J Surg 2004. 3. Lakey et al. Ann Pharmacother 2009. 4. Phelan et al (in review). 5. AMA Driver Guide, http://www.ama-assn.org/ama/pub 6. Scanlan et al. Am J Geriatr Psychiatry 2007 © 3-11 Soo Borson MD
Essential Clinical and Administrative Skills • Timely identification and accurate diagnosis of cognitive impairment • Comfort with difficult discussions (e.g. diagnosis, driving, moving) • Individualized health care plans for long-term palliation • Planned collaboration with caregivers, care managers and specialists • Effective use of targeting and management tracking tools © 3-11 Soo Borson MD
Screening for Cognitive Impairment in Primary Care: RCT • Four similar clinics in the same network, 2 randomized to screening, 2 to usual practice • QI framework – patient consent not required • After vital signs, MA administered the Mini-Cog • Reliability high • Refusals rare (<2%) • N = 524 screened (70% of patients age 65+ in eligible clinic panels) • 18% of patients screened positive Borson S et al JGIM 2007 © 3-11 Soo Borson MD
Impact of Routine Screeningon Physician Practice Borson S et al JGIM 2007
5-Year Follow On In progress: Comparison with age-matched older adults screening negative 5 years earlier DeMers S et al. AAGP Annual Meeting, Honolulu, 2009 © 3-11 Soo Borson MD
Screening for Cognitive Impairment: Policy Update • US Preventive Services Task Force • To update evidence and recommendations this year • New Medicare benefit: Annual Wellness Visit (effective Jan 2011) • Cognitive assessment for early detection • Personalized health risk assessment (HRA) and prevention plan • Incentives • For patients: no deductible or co-pay • For physicians: reimbursement equivalent to Level 4 E/M Fact sheet available on www.alz.org © 3-11 Soo Borson MD
Cognitive Assessment in the AWV • No method specified by CMS • Acceptable pathways can include • A screening test • A question about cognition to the patient and/or family • A spontaneous patient or family concern about the patient’s cognition • Any/all of these pathways will generate a cohort of patients whose cognitive status should be further evaluated • A ‘cognitive visit’ can then be scheduled
Clinical history Basis for concern First symptoms and signs Context of emerging or worsening Pattern of progression Functional deficits (advanced IADL; IADL, basic self care ADL) Brief neurological exam Look for informative signs that suggest etiology Confirmatory cognitive testing What’s in a “Cognitive Visit”?
Risk factor review • Clinical vascular disease • Head injuries • Complications of surgery • Neurotoxins • Prescription and OTC medications • Family history • Recent hospitalization for acute or critical illness1 or complex surgical procedure 1 Ehlenbach et al JAMA 2010 © 3-11 Soo Borson MD
Further Workup • Use blood tests selectively • Mainly for treatable confounders and problems related to effects of dementia • Few dementias have specific clinical lab indicators (e.g., HD, HIV, STD) • Think about neuroimaging • Few patients require it for diagnosis • Create a short list of most likely diagnoses • If you’re not sure, consider specialty consultation © 3-11 Soo Borson MD
Diagnosis and Disclosure • Whose responsibility? • May share with a specialist • How to do it? • Patient-centered communication • Patient’s thoughts, feelings, fears • Caregiver’s knowledge and concerns • Physician’s positive affect, direct language, optimism • When to follow up? • Anticipate adjustment period • See a month or less after the diagnosis – check in • Answer questions, respond to concerns • Refine management and follow up plan Boise et al, Gerontol 1999; Iliffe et al, Int J Geriatr Psychiatry 2009; Eccles et al, Int J Behav Med 2009; Zaleta and Carpenter Am J Alz Other Dem 2010 © 3-11 Soo Borson MD
Next Steps: Prepare for Chronic Care Data on Alzheimer’s disease from Group Health Cooperative ADPR/ACT studies (n = 521). Larson EB et al. Ann Intern Med 2004. Most other studies find much shorter survival, since diagnosis occurs later. © 3-11 Soo Borson MD
Integrate Dementia • Palliative philosophy from diagnosis to death, since dementia is a… • Target of treatment • Modifier of care for other conditions • Prognostic indicator • Risk indicator • Care is stage-specific • Components of palliation vary over time • Care is always a collaboration • You, the patient, and the family • A medical dementia specialist, when needed • A psychosocial care manager, especially at moderate dementia stages and beyond, or when families are stressed © 3-11 Soo Borson MD
Problems Peak at Different Times in the Course of AD 100% Cognitive ability Functional ability Behavioral problems Caregiver time demand/stress Change with disease progression Stage and duration of usual clinical trials of antidementia drugs 0% 0 1 2 3 4 5 6 7 8 9 Years from symptom onset
Stage-Specific Management Concepts • Very early stage (“MCI”) – educate, support healthy habits, prevent 2O and 3O complications, re-evaluate cognition ove4r time, discuss end of life preferences • Mild to moderate stage – treat dementia, find and manage risks, set goals for comorbid chronic conditions, support good caregiver-patient dynamics and regular medical f/u; bring secondary family members in; review end of life wishes; encourage legal review (DPOA for finances and health care, will, POLST) © 3-11 Soo Borson MD
Moderate to severe stage – 24 hr supervision and shared caregiving; prevent injury, expect behavioral problems, hospitalizations, and caregiver burnout; review and simplify medications; surgery only for urgent conditions with favorable prognosis; update POLST • Advanced and terminal stage – remove unnecessary medications; update POLST; provide hospice/comfort care; with caregivers, plan for possible terminal event scenarios and actions appropriate to those – the ‘what if’ conversation
Diagnosis and Staging Neurobehavioral Assessment & Management Medical Comorbidity and Risk Management Patient Caregiver Assessment, Counseling, Services, and Planning A Comprehensive Framework for Dementia Care
Operationalizing the Model • Dementia as a disease • Diagnose etiology /type • Establish stage (cognitive, functional) • Consider cognitive enhancing medications • Support adjustment to diagnosis • Anticipate risks specific to types/stages of dementia • Neuropsychiatric probems • Recognize depression, demoralization, loss of confidence, anxiety, agitation, aggression, psychosis • Analyze behavioral problems – causes and consequences • Implement practical psychosocial interventions • Train caregivers in hands-on prevention and management • Use psychotropic medications selectively • Comorbid medical conditions and risks • Manage to protect the brain • Identify/implement adherence supports • Address key safety issues (e.g. driving, falls, injury potential) • Reframe goals to match prognosis/stage • Coordinate care with other providers • Palliation at every stage • Caregiver issues • Encourage realistic expectations • Assess and respond to stress and burden • Identify caregivers needing community based services, refer, and follow up • Track ongoing needs and gaps • Provide clinical options to optimize adjustment across stages © 3-11 Soo Borson MD
Measuring the Quality of Dementia Care • Patient and practice level • ACOVE-3 indicators • Emerging consensus measures (AMA) • Health system level • Uptake of annual wellness visits and their cognitive assessment component • Reduction in avoidable hospitalizations and post-hospital readmissions © 3-11 Soo Borson MD
ACOVE-3 Dementia QIs • Cognitive and functional screening/evaluation • Medication review and adjustment • Neurological assessment • Lab testing (including HIV if at risk) • Depression screening • Cholinesterase inhibitor discussion • Behavioral symptoms of dementia • Stroke prophylaxis • Caregiver support and patient safety • Driving (state law variations) • Restraint documentation and communication (hospital) Feil et al. JAGS 2007. © 3-11 Soo Borson MD
AMA Consensus Performance Measures • AMA PCPI with AAN, AGS, AMDA, and APA/AAGP – for patients with a dementia diagnosis • 10 domains of quality • Dementia staging • Cognitive assessment • Functional status assessment • Neuropsychiatric symptom assessment • Screening for depressive symptoms • Management of neuropsychiatric symptoms • Counseling about safety matters • Counseling about driving • Comprehensive end of life counseling/advance care planning • Caregiver education and support © 3-11 Soo Borson MD
Setting Up a Care Collaborative • Dementia Care Manager (DCC) Models • Callahan et al. JAMA 2006 • Interdisciplinary team led by an advanced practice nurse • Vickrey et al. Ann Internal Med 2006 • Dementia care guideline model, non-medical care managers in a primary care setting, involvement of Alzheimer’s Association and social care agencies • Primary Care Practice Redesign • Reuben et al. JAGS 2010 • Six components, internal practice change + Alzheimer’s Association • Specialty-Based Medical Home Model • Lessig et al. JAGS 2006 • Cooperative Dementia Care Clinics and Dimensional Approach to Care © 3-11 Soo Borson MD
Advanced Practice Nurse Model (Callahan et al.) © 3-11 Soo Borson MD
Dementia Care Guideline Model (Vickrey et al.) © 3-11 Soo Borson MD
Common to These Models • Patient eligibility defined by diagnosis of dementia and participation of a family caregiver • Addition of psychosocial management options • Care partnership with the family • Specified communication pathways • Tools for measuring outcomes • Relatively small effect sizes
Finding High-Needs Patients and Caregivers • Goal: predict service needs and gaps by data easily acquired in primary care • Community sample of 215 patient/caregiver pairs • Dementia-related services needed/used in past year, 8 physician-initiated and 8 psychosocial case manager-initiated. Scored as # needs and # gaps. • Caregiver stress (1 item, scored 1-5) and # of patient behavior problems (5 items, scored 0-5) • Result: stress and behavior problems by far the strongest predictors of service needs and gaps © 3-11 Soo Borson MD
Services: Physician Management Low behavior problems High behavior problems
Services: Psychosocial Care Management Low behavior problems High behavior problems
Screen: Caregiver Stress + Patient Behavior High stress + >1 behavior problems Low to moderate stress + >1 behavior problems Low to moderate stress + 0-1 behavior problems Urgent, intensive physician/case manager collaboration May need geropsychiatrist Primary Care Refer to case manager Primary Care Encourage reporting of new problems © 3-11 Soo Borson MD
Physician-Based Medical Home(Lessig et al) © 3-11 Soo Borson MD
Improving Care:Moving Into the Medical Home Neighborhood • Patient Centered Medical Home • Central hub for information, primary care, and care coordination for a defined group of patients • Each patient has a personal physician who directs a team • Collective responsibility for the patient’s health care • Patient Centered Medical Neighbor • Specialty/subspecialty practice committed to collaboration with a PCMH • Standards for linking with a PCMH • For some patients, PCMN physician may provide the PCMH Laine, Sinsky, Lee: Ann Intern Med 2011 © 3-11 Soo Borson MD
Thanks to…Mary Lessig BSJim Scanlan PhDShaune DeMers MDPeter Vitaliano PhDJeff Hummel MD, MPHKathy Gibbs RN, CNSTeresa Holder MSWBeth Zuhr BAand our residents and fellows whose training turned the practice into words