Download
1 / 38
380 likes | 486 Views
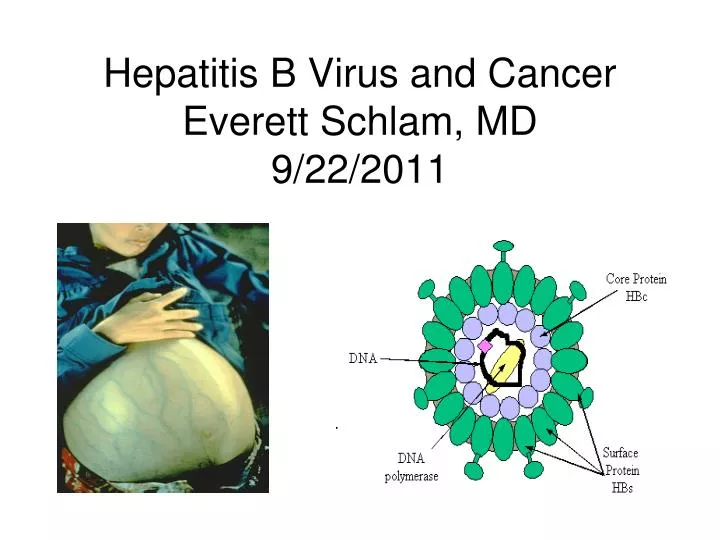
Hepatitis B Virus and Cancer Everett Schlam, MD 9/22/2011. Pick any number between 2 and 10 Multiply that number x 9 Add the two digits of that number together Subtract 5 from that number Pick the letter which corresponds to that number in the alphabet Ie, A=1 B=2 C=3 D=4

E N D
Pick any number between 2 and 10 • Multiply that number x 9 • Add the two digits of that number together • Subtract 5 from that number • Pick the letter which corresponds to that number in the alphabet Ie, A=1 B=2 C=3 D=4 • Pick a country which begins with that letter. • Now take the second letter of that country and choose a large animal which begins with that letter
Viral Hepatitis 5 types: A: fecal-oral transmission B: sexual fluids & blood to blood C: blood to blood D: travels with B E: fecal–oraltransmission Vaccine Preventable Adapted from Corneil, 2003
Hepatitis B • Epidemic jaundice described by Hippocrates in 5th century BC • Jaundice reported among recipients of human serum and yellow fever vaccines in 1930s and 1940s • Australia antigen described in 1965 • Serologic tests developed in 1970s
Hepatitis B Complications • Fulminant hepatitis • Hospitalization • Cirrhosis • Hepatocellular carcinoma • Death
Hepatitis B Virus Infection • More than 350 million chronically infected worldwide • Established cause of chronic hepatitis and cirrhosis • Human carcinogen—cause of up to 80% of Hepatocellular carcinomas • More than 600,000 deaths worldwide in 2002
Only 20% will show symptoms Initially ! Natural History of Hep C 20% Clear the Virus Chronic Infection Acute Infection Healthy Liver 80% Virus Continues to Damage Liver Adapted from Lauer and Walker, NEJM 2001
Natural History Con’t Liver Cancer 1-4%/year Cirrhosis 20-30% Chronic Hepatitis Most symptoms begin to show only when liver is more severely damaged
Factors Affecting Progression • 30yrs or longer if: • Young at time of infection • Healthy liver at time of infection • Female • 20yrs or less if: • Drinking alcohol • Co-infection (HIV, Hep B) • Damaged liver before infection Adapted from Bigham, BC Hepatitis Services 2002
IDU/snorting (51%) No RF identified (23%) Incarceration (3%) Transfusion/dialysis blood contact (4%) HCV-infected household member/sexual partner (7%) Hospitalization dental work (6%) Tattooing piercing (6%) Risk Factors Source: Health Canada Enhanced Surveillance, Oct 98-Oct 99, Calgary, Edmonton, Winnipeg, Ottawa
Overall cure rate with new treatment is 55% * Hepatitis C • Affects each person differently • No vaccine available • Many people have the virus and do not even know it *BC Hepatitis Service 2003
Hepatitis C Dispelling Myths • Hepatitis C is not spread by: • Casual contact • Hugging/kissing • Sharing eating utensils and drinking glasses • Sneezing/coughing • Shaking hands • Sitting on a toilet seat
HBV Disease Burden in the United States • Pre-vaccine era • estimated 300,000 persons infected annually, including 24,000 infants and children • 2005 • estimated 51,000 infections • Overall cure rate about 55%
Hepatitis B Perinatal Transmission* • If mother positive for HBsAg and HBeAg • 70%-90% of infants infected • 90% of infected infants become chronically infected • If positive for HBsAg only • 5%-20% of infants infected • 90% of infected infants become chronically infected *in the absence of postexposure prophylaxis
Strategy to Eliminate Hepatitis B Virus Transmission—United States • Prevent perinatal HBV transmission • Routine vaccination of all infants • Vaccination of children in high-risk groups • Vaccination of adolescents • Vaccination of adults in high-risk groups
Risk Factors for Hepatitis B CDC Sentinel Sites. 2001 data.
Hepatitis B VaccineLong-term Efficacy • Immunologic memory established following vaccination • Exposure to HBV results in anamnestic anti-HBs response • Chronic infection rarely documented among vaccine responders
Adults at Risk for HBV Infection • Sexual exposure • sex partners of HBsAg-positive persons • sexually active persons not in a long-term, mutually monogamous relationship* • persons seeking evaluation or treatment for a sexually transmitted disease • men who have sex with men *persons with more than one sex partner during the previous 6 months
Adults at Risk for HBV Infection • Percutaneous or mucosal exposure to blood • current or recent IDU • household contacts of HBsAg-positive persons • residents and staff of facilities for developmentally disabled persons • healthcare and public safety workers with risk for exposure to blood or blood-contaminated body fluids • persons with end-stage renal disease
Prevaccination Serologic Testing • Not indicated before routine vaccination of infants or children • Recommended for • all persons born in Africa, Asia, the Pacific Islands, and other regions with HBsAg prevalence of 8% or higher • household, sex, and needle-sharing contacts of HBsAg-positive persons • HIV-infected persons • Consider for • Groups with high risk of HBV infection (MSM, IDU, incarcerated persons)
What are the recommended serological screening tests for Hepatitis B?
Screening Tests for Hepatitis B • HBsAg • Anti-HBs • Cost for both tests about (150-250 dollars) • Further testing and treatment determined by results of HBsAG and Anti-HBs
Chronic Inactive Hepatitis B Infection • Surveillance monitoring for reactivation
Chronic Active Hepatitis B Treatment Options • Interferons • Interferon alfa-2b • Peginterferon alfa 2-b • Nucleotids(t)ide analogs • Lamivudine • Adenovir • Entecavir • Telbivudine • Tenofovir
Who is post vaccination serological testing recommended for and when should the testing be performed?
Postvaccination Serologic Testing • Not routinely recommended following vaccination of infants, children, adolescents, or most adults • Recommended for: • Infants born to HBsAg+ women • Hemodialysis patients • Immunodeficient persons • Sex partners of persons with chronic HBV infection • Certain healthcare personnel
Healthcare personnel who have contact with patients or blood should be tested for anti-HBs (antibody to hepatitis B surface antigen) 1 to 2 months after completion of the 3-dose series Postvaccination Serologic Testing
Management of Nonresponse to Hepatitis B Vaccine • Complete a second series of three doses • Should be given on the usual schedule of 0, 1 and 6 months • Retest 1-2 months after completing the second series
Persistent Nonresponse to Hepatitis B Vaccine • Less than 5% of vaccinees do not develop anti-HBs after 6 valid doses • May be nonresponder or "hyporesponder" • Check HBsAg status • If exposed, treat as nonresponder with postexposure prophylaxis
Needle Prick • Do not “milk” prick site • Wash the area with soap and water • Go to nearest emergency department for assessment and treatment
Chronic Hepatitis B and risk of Hepatocellular Cancer • Hepatocellular Cancer occurs in up to 25% of men and 15% of women over their lifetimes
Hepatitis B and Cancer • Hepatocellular Cancer is a devastating complication of Hepatitis B • Prevention is the optimal strategy to prevent acquisition of Hepatitis B • Immunization and avoidance of high risk activities are of upmost importance