Download

1 / 25
260 likes | 474 Views
Nouveaux Antithrombotiques en Prophylaxie de MTEV. Bruno TRIBOUT Médecine Vasculaire CHU Amiens. www.thrombose-picardie.com. Patients chirurgicaux à très haut risque MTEV : ACCP 2004. Chirurgie chez patients avec multiples F de R âge > 40 ans, cancer, ATCD de TEV

E N D
Nouveaux Antithrombotiquesen Prophylaxie de MTEV Bruno TRIBOUT Médecine Vasculaire CHU Amiens www.thrombose-picardie.com
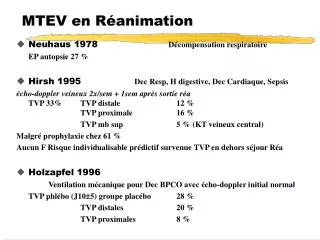
Patients chirurgicauxà très haut risque MTEV : ACCP 2004 • Chirurgie chez patients avec multiples F de R âge > 40 ans, cancer, ATCD de TEV • PT Hanche, PT Genou, fracture hanche • Polytraumatisé sévère, traumatisme médullaire Risque TEV sans prophylaxie TVP surale 40 – 80% TVP proximale 10 – 20% EP symptomatique 4 – 10% EP fatale 0,2 – 5% Prophylaxie : HBPM risque élevé, Fondaparinux Geerts WH Chest 2004;126:338S-400S
Mélagatran Thrombine
Bénefice/Risque Antithrombine directe(Xi)Mélagatran Evènements Thromboemboliques veineux majeurs (%) Hémorragies Majeures (%) 8 6,2 6,3 5,7 6 3,6 3,3 4 2,3 1,7 1,4 1,2 1,2 0,9 0,8 2 0 US 237 METHRO III EXPRESS US 237 METHRO III EXPRESS Ximelagatran Enoxaparin
Dabigatran EtexilateAntithrombine directe Dabigatran etexilate : prodrogue Dabigatran : antithrombine
Dabigatran EtexilatePharmacologie (1) • Prodrogue convertie en Dabigatran par estérases • Dabigatran : antithrombine directe réversible • Délai pic Tmax Dabigatran < 2h • T1/2 : dose unique 810h ; dose multiple 14 17h • Administration 1 ou 2 prises/j • Biodisponibilité : 6 à 7% • Elimination rénale > 80% : excrétion inchangée dans les urines • Aucun antidote dialysable Stangier 2005-2007-2008 Blech 2007 Rely-trial.com Eikelboom 2007 Weitz 2007
Dabigatran EtexilatePharmacologie (2) • Délai pour chirurgie : 12h après dernière prise • Elimination : 12 h après -50% ; 24h après -75% • Alimentation : retarde absorption, réduit variabilité interindividuelle • Aucune implication Cytochrome P450 • Interaction médicamenteuse : pantoprazole IPP IPP réduit absorption : biodisponibilité -20% • Insuffisance rénale FG < 50 ml/mn → élimination rénale ; exposition AUC Contre-indication : FG < 30 ml/mn (Eriksson Lancet 2007) Stangier 2005-2007-2008 Blech 2007 Rely-trial.com Eikelboom 2007 Weitz 2007
Hépatotoxicité ?Dabigatran Etexilate • Essai PETRO : phase II recherche de dose Fibrillation auriculaire non valvulaire Dabigatran E : 50 – 150 – 300mg 2x/j per os vs Warfarine Durée 3 mois Dabigatran E Warfarine Transaminases > 3N 3 mois 4/432 0,9% 0/70 6 mois 1,5% Bilirubine > 2N 0/432 Ezekowitz MD Am J Cardiol 2007;100:1419-1426
Dabigatran Etexilate BISTRO II (1)Europe II recherche dose PTH-PTG PTG : 32% PTH : 68% phlébographie 610j médiane= 7j 1ère dose 14h post-op1èredose12h pré-op DE 50mg DE 150mg DE 300mg DE 225mg Enoxaparine 40mg/j 2x/j 2x/j 1x/j 2x/j Efficacité : ETEV totaux → dose dépendante (N= 1464)p< 0,0001 28,5% 17,4% 16,6% 13,1% 24,0% NS OR= 0,65 OR=0,61 OR= 0,47 TVP proximales 5,0% 3,3% 2,1% 1,7% 5,6% Tolérance : hémorragies majeures → dose dépendante (N= 1949) 0,3% 4,1% 3,8% 4,7% 2,0% Dose optimale entre 100 et 300mg/j Identité pour dose 300mg/j entre 1 prise ou 2 prises/j Eriksson BI J Thromb Haemost 2005;3:103-111
Dabigatran Etexilate BISTRO II (2)Europe II recherche dose PTH-PTG PTG : 32% PTH : 68% phlébographie 610j médiane= 7j 1ère dose 14h post-opmédiane= 2,6h1èredose12h pré-op DE 50mg DE 150mg DE 300mg DE 225mg Enoxaparine 40mg/j 2x/j 2x/j 1x/j 2x/j Analyse post-oc : effet délai 1ère dose post-op 2h > 2h Efficacité 14,1%22,4%p= 0,0005 Tolérance NS Eriksson BI J Thromb Haemost 2005;3:103-111
Dabigatran Etexilate RE-MODEL Europe III PTG phlébographie 610j : 8 ± 2j 1ère dose 14h post-opà demi-dose1èredose12h pré-op DE 150mg po 1x/j DE 220mg po1x/j Enoxaparine sc 40mg/j Efficacité : ETEV totaux + Mortalité globale (N= 1541) 40,5% 36,4% 37,7% NI TVP proximales + EP 3,8% 2,6% 3,5% NS Tolérance : hémorragies majeures (N= 2076) 1,3% 1,5% 1,3% NS Non infériorité pour 2 doses DE Eriksson BI J Thromb Haemost 2007;5:2178-2185
Dabigatran Etexilate RE-MOBILIZENord-Americain III PTG N= 2615 phlébographie 1215j 1ère dose 612h post-opà demi-dose1èredose12-24h post-op DE 150mg po 1x/j DE 220mg po1x/j Enoxaparine sc 30mg 2xj Efficacité : ETEV totaux + Mortalité globale 33,7% 31,1% 25,3% p=0,0009 vs E p= 0,02 vs E supériorité HBPM ETEV majeurs : TVP proximales + EP + décès TEV 3,0% 3,4% 2,2% NS Tolérance : hémorragies majeures 0,6% 0,6% 1,4% NS Essai de non-infériorité pour 2 doses DE Friedman RJ ISTH2007
Dabigatran Etexilate RE-NOVATE III Europe Prophylaxie prolongée PTH Non-infériorité phlébographie 2835j médiane= 33j 1ère dose 1-4h post-opà demi-dose1èredose12h pré-op DE 150mg po 1x/j DE 220mg po1x/j Enoxaparine sc 40mg/j Efficacité : ETEV totaux + Mortalité globale (N= 2651) 8,6% 6,0% 6,7% NI ETEV majeurs : TVP proximales + EP + décès TEV (N= 2714) 4,3% 3,1% 3,9% NS Tolérance : hémorragies majeures (N= 3463) 1,3% 2,0% 1,6% NS Hépatotoxicité : Transaminases > 3N 3% 3% 5% p= 0,008 Délai 1ère dose DE médiane= 3,4h Eriksson BI Lancet 2007;370:949-956
RivaroxabanPharmacologie (1) • Anti-facteur Xa direct : site actif • Délai pic Tmax : 2 à 4h • T1/2 : 59h → sujet âgé : 11 13h • Administration 1 ou 2 prises/j • Biodisponibilité orale 80% • Excrétion rénale prédominante 66% excrétion inchangée dans les urines : 36% dose fécale/biliaire : 28% • Aucun antidote Turpie ATVB2007 Eikelboom Circulation2007 Hirsh Circulation2007
RivaroxabanPharmacologie (2) • Alimentation : absorption variabilité interindividuelle • Interactions médicamenteuses Inhibiteurs Cytochrome P450 : CYP3A4 kétokonazole, macrolides, antiprotéases VIH • Hépatotoxicité : cytolyse hépatique risque faible Turpie ATVB2007 Eikelboom Circulation2007 Hirsh Circulation2007
RivaroxabanPharmacologie (3) : sujet âgé Rivaroxaban : dose unique orale 10mg Sujets âgés > 75 ansversus contrôles 18-45ans • Cl totale et rénale rivaroxaban corrélation positive FG ; corrélation négative âge • AUC[rivaroxaban]p141% ; AUC[act antiXa]p158% corrélation négative FG Kubitza D ASH2006 ISTH2007
RivaroxabanPharmacologie (4) : insuffisant rénal Rivaroxaban : dose unique orale 10mg N= 32 FG 80ml/mn 50-79 ml/mn 30-49 ml/mn FG < 30 ml/mn AUCRp 100% 144% 152% 164% p< 0,05 AUCAXap 100% 150% 186% 200% p< 0,01 corrélation R= -0,49 Excrétion urinaire R (% dose) : Cl rivaroxaban FG 29% 20% 13% 10% Ajustement posologique ? Halabi A ASH2006
Rivaroxaban : recherche dose phase II1 prise/j PTH-Europe ODIXa-HIP Phlébographie J6 à J10 Efficacité : ETEV totaux Mortalité N= 618 Tolérance : Hémorragies majeures N= 845 25% Efficacité p=NS 4,9% Tolérance p< 0,04 40mg/j 1ère dose 12h pré-op 1ère dose 6-8h post-op Choix 10mg 1x/j Eriksson BI Circulation 2006;114:2374-2381
Rivaroxaban RECORD 1 Europe III Prophylaxie prolongée PTH Phlébographie : 35 ± 4j Rivaroxaban 10mg 1x/j versus Enoxaparine 40mg 1x/j 1ère dose per os 6-8h post-op 1ère dose sc 12h pré-op Efficacité : ETEV totaux + mortalité (n= 3153) 1,1% RRR= 70% p< 0,001 3,7% ETEV majeurs : TVP prox, EP, décès TEV 0,2% RRR= 88% p< 0,001 2,0% Tolérance : hémorragies majeures (n= 4433) 0,3% NS 0,1% Eriksson BI ASH2007
Rivaroxaban RECORD 2 Europe III Prophylaxie PTH : prolongée courte Phlébographie : 35 ± 4j Rivaroxaban 10mg 1x/j versus Enoxaparine 40mg 1x/j 1ère dose per os 6-8h post-op 1ère dose sc 12h pré-op Durée : 35 ± 4j Durée : 10 à 14j Efficacité : ETEV totaux + mortalité (n= 1733) 2,0% RRR= 79% p< 0,001 9,3% ETEV majeurs : TVP prox, EP, décès TEV 0,6% RRR= 88% p< 0,001 5,1% Tolérance : hémorragies majeures (n= 2457) 0,1% NS 0,1% Kakkar AJ ASH2007
Rivaroxaban RECORD 3 Europe III Prophylaxie PTG : 10 à 14j Phlébographie : 13 ± 2j Rivaroxaban 10mg 1x/j versus Enoxaparine 40mg 1x/j 1ère dose per os 6-8h post-op 1ère dose sc 12h pré-op Efficacité : ETEV totaux + mortalité (n= 1702) 9,6% RRR= 49% p< 0,001 18,9% ETEV majeurs : TVP prox, EP, décès TEV 1,0% RRR= 62% p< 0,02 2,6% TEV symptomatiques 0,7% RRR= 62% p= 0,005 2,0% Tolérance : hémorragies majeures (n= 2459) 0,6% NS 0,5% Lassen MR ISTH2007 ASH2007
Registre ESCORTEFracture de hanche • Registre prospectif multicentrique France 10-11/2002 ; suivi 6 mois N= 6860 patients consécutifs • Médiane âge : 82 ans • Prophylaxie par HBPM péri-opératoire 98% prolongée 4 semaines 69,5% • TEV symptomatiques à 3 mois : 1,3% • Hémorragies majeures : 1,2% • Mortalité à 6 mois : 15% [causes cardiovasc : 27%] • Insuffisance rénale sévère FG 30 ml/mn : 16% F de R hémorragies majeures : Insuffisance rénale p< 0,001 Rosencher N J Thromb Haemost 2005;3:2006-2014
MTEV : populations spéciales • Canada : Montreal, London hôpitaux universitaires(04/2004→ 03/2005) • N= 524 patients TVP: 81% EP: 19% • Sujet âgéâge moyen: 62ansâge > 75 ans 31% âge > 80 ans 18% • Insuffisance rénale FG : 30 60 ml/mn 20% FG : 30 50 ml/mn 11% FG < 30 ml/mn 5% • Obésité poids > 100kg 15% • Cancer évolutif 26% Cook L ASH 2006 ISTH 2007
Sujet âgé Insuffisance rénaleNational Kidney Foundation • Age : 60-69 ans Albuminurie 18% FG < 60ml/mn 7% • Age 70 ans Albuminurie 30% FG < 60ml/mn 26% Stevens LA Levey ASN Engl J Med 2005;352:2122-2124