Download
1 / 102
1.02k likes | 1.05k Views
The Medical Patient The Renal System; Hypertensive Emergencies. Condell Medical Center EMS System ECRN Packet Module IV 2008 CE. Prepared by: Sharon Hopkins, RN, BSN, EMT-P. Objectives. Upon successful completion of this module, the ECRN should be able to:

E N D
The Medical Patient The Renal System; Hypertensive Emergencies Condell Medical Center EMS System ECRN Packet Module IV 2008 CE Prepared by: Sharon Hopkins, RN, BSN, EMT-P
Objectives • Upon successful completion of this module, the ECRN should be able to: • List the components and function of the urinary system • State signs and symptoms of chronic kidney disease • Define hemodialysis • Identify the differences between AV fistulas and AV shunts & implications in the field • Apply the Renal SOP’s given a scenario • List the steps in performing an abdominal assessment
Describe the physical assessment of the patient with flank pain • Describe the management of the patient with flank pain • Define the criteria for a hypertensive emergency • List the signs and symptoms of hypertensive emergencies • Describe the rationale for treatment using Lasix and Nitroglycerin for hypertensive emergencies • Describe the proper technique to obtain a blood pressure • Describe the components of a neurological assessment
Successfully calculate the GCS given the findings of the patient assessment • Identify proper method of pupillary assessment • Identify the preparation of an Amiodarone IVPB set-up in the field per Region X SOP’s • Identify and appropriately state interventions for a variety of EKG rhythms • Identify ST elevation on a 12 lead EKG • Successfully complete the 10 question quiz with a score of 80% or better
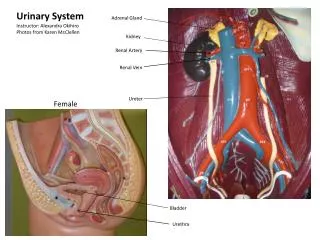
Urinary System • Contains 4 major structures • Kidneys • Vital organs • Located in upper abdomen; retroperitoneal area • 1 behind the spleen; 1 behind the liver • Ureters • Urinary bladder • Urethra
Function of the Urinary System • Major functions • Maintains blood volume via proper balance of water, electrolytes, and pH • Retains key compounds (ie: glucose) and eliminates wastes (ie: urea) • Monitors and maintains arterial blood pressure (in addition to other mechanisms) • Regulates erythrocyte (RBC) development
Urinary Bladder • Storage receptacle for the production of urine until it is convenient or necessary to void • Fully distended can hold 500 ml of urine • The more distended the bladder, the more vulnerable to blunt trauma • After urination, the bladder contains about 10 ml of fluid
Chronic Kidney Disease • Can be from a specific kidney disease or as a complication from other conditions • Diabetes • #1 reason in USA for need for kidney transplant • Hypertension • Kidney inflammation (glomerulonephritis) • Inflammation of blood vessels (vasculitis) • Polycystic kidney disease
Chronic Kidney Disease • Diseased or injured kidneys • Blood flow through the renal system decreases • Inflammatory changes occur in the glomeruli • A group of capillaries where blood is filtered into a nephron (structure that produces urine) • Capillary walls thicken decreasing permeability • Glomerular filtration rate (GFR) is reduced • Volume of blood filtered per day thru glomeruli
Symptoms of Chronic Kidney Disease • Most common symptoms • Swelling, usually of lower extremities • Fatigue • Weight loss, loss of appetite • Nausea and/or vomiting • Change in urination • Reduction in volume or frequency • Change in sleep patterns • Headache • Itching – high levels of phosphorus in system; dry skin • Difficulties with memory or concentration
Complications of Chronic Kidney Disease • Hypertension • May be a leading cause but can also develop in the early stages as a complication • Anemia • Decreased production of red blood cells • Bone disease • Disorders of calcium and phosphorus • Malnutrition • Altered functional status and well-being
Dialysis • Dialysis is required when the kidneys fail and a transplant is not performed • Peritoneal dialysis uses a catheter thru the abdominal wall to filter the blood
Hemodialysis • Hemodialysis is a procedure in which a machine filters harmful waste and excess salt and fluid from your body • Access points are created to be functional within weeks and to last several to many years • Usual access point is the forearm
Fistulas and Shunts • Arteriovenous (AV) fistula • Most common type of access • Fistula created internally by sewing an artery to a vein forming a small opening between the two • Pressure from the arterial flow eventually enlarges and strengthens the vein • May take 6 weeks to heal but can last for years
Arteriovenous (AV) graft • Access is similar to a fistula • A synthetic tube is used to surgically connect the artery to the vein • AV grafts often heal within 2-3 weeks • With proper care, can last several years • Higher likelihood of forming clots or becoming infected than an AV fistula
Hemodialysis • Most people treated with hemodialysis 3 times a week • Each session lasts approximately 3-5 hours • Some patients, at some dialysis centers, may choose daily dialysis • Usually performed 6 days per week for 2 – 21/2 hours each session • Patients often report improved B/P and quality of life with the more frequent dialysis
Continuous Ambulatory Peritoneal Dialysis • CAPD is a self-care treatment where the patient instills dialysate fluid into the peritoneal (abdominal) cavity through a surgically implanted catheter through the abdominal wall • The dialysate stays in the abdominal cavity a prescribed period of time and then is drained out
CAPD Instructions • EMS will not disconnect the CAPD bags from the catheter • If the patient is transported, transport is with the drainage bag remaining below the level of the patient’s waist • EMS will not infuse any fluids or medications directly into the catheter • This IS NOT an alternate IV site
Region X Renal ProtocolCare of Patients with Grafts or Shunts • Do NOT take B/P on arm with active fistula or graft • Do NOT start IV on arm with active fistula or graft • If site is bleeding, apply direct pressure • In case of arrest and no extremity IV access, consider external jugular or IO site • EMS access of fistula or graft is only after contact with Medical Control who will give directions
Care of The Renal Patient • Best to err on the side of conservative treatment • Monitor and support the ABC’s • High flow O2 is appropriate to maximize respiratory efficiency • Monitor fluid administration carefully • Monitor cardiac rhythm for disturbances • Home caregivers will be a great resource of information for the equipment used
Abdominal Pain Assessment • Chief complaint • The sign or symptoms that prompted the patient to call for or seek help • Use an open – ended question to determine the reason for the patient seeking help • “Why are you here today?” or • “What seems to be the problem?” • During the interview the chief complaint generally becomes more specific
OPQRST Assessment Mnemonic • O – onset of the problem • Did problem start suddenly or gradually? • What was patient doing at the time? • P – provocation/palliation • What makes the symptoms worse? Better? • Q – quality • In the patient’s own words how do they describe their pain (ie: crushing, tearing, sharp, dull?)
R – region/radiation • Where is the symptom? • Does it move? • If the patient uses one finger or isolates to one spot, the pain is considered localized • If the pain is described using both hands or indicating a larger area, the pain is diffuse • Is there referred pain (pain felt in a body area away from the source)?
S – severity • Intensity of pain or discomfort • 0 – 10 scale • “0” is no pain; “10” is the worse pain in your life • Can the patient be distracted? • Do they lie still or are they writhing about? • T – time • When did the symptoms begin?
Associated symptoms • Are other symptoms present that are commonly linked to certain diseases that can help rule in or out your diagnosis? • Pertinent negatives • Are any likely associated symptoms absent? • Absence of symptoms can be information as helpful as presence of other symptoms
Assessment Pitfalls in the Chronic Renal Patient • The challenge to the medical professional is to separate the acute complaint from the chronic condition • What is new today that changes your status? • Many patients with chronic renal disease have unstable baselines to start with • Fluid and electrolyte imbalance • EKG disturbances
Physical Assessment - Abdomen • Boundaries run from xiphoid process to symphysis pubis • A full bladder will distort assessment and increase discomfort for the patient • To relax the abdominal wall or to ease pain, a pillow placed under the knees would be helpful • Start by asking the patient where it hurts • Examine painful areas last
Warm your hands and stethoscope • If hands are cold, palpate over clothing until hands warm up • Monitor facial expressions for pain or discomfort • Validate the facial expression • Often the patient may scrunch their face in anticipation of pain • Assessment techniques to use • Inspection, auscultation, percussion, lastly palpation
Abdominal Assessment Techniques • Inspection • A visual review looking for abnormalities • Always performed first for all assessments • Auscultation • Move the stethoscope in a circle approximately 2 inches from the umbilicus listening for bowel sounds • Normal bowel sounds gurgle approximately every 5-15 seconds
Percussion • Not often performed in the field • Helps determine size and location of organs • Determines gas, solid, and fluid filled areas • Tympany heard over most of abdomen • Dullness percussed over spleen and liver
Palpation • Palpate painful areas last • To increase comfort to patient, have them take slow, deep breaths thru open mouth • Flexing knees relaxes abdominal wall • Abdominal pain on light palpation indicates peritoneal irritation or inflammation • Voluntary guarding – patient anticipates pain or is not relaxed • Involuntary guarding – peritoneal inflammation (lining of abdominal cavity)
Region X SOP - Abdominal Pain Stable Patient • Routine medical care • Watch the patient for vomiting • Stable patient • Patient alert • Skin warm and dry • Systolic B/P > 100 mmHg • Contact Medical Control for pain management (Region X carries Morphine)
Region X SOP - Abdominal Pain Unstable Patient • Routine medical care • Watch the patient for vomiting • Unstable patient • Altered mental status • Systolic B/P < 100 mmHg • Establish IV; x2 if possible • Fluid challenge in 200 ml increments • Carefully monitor breath sounds • 20 ml/kg in pediatric patient (max 3 challenges) • Contact Medical control for pain management
Flank Pain • Where’s the flank? • The area of the back below the ribs and above the hip bones • What organs lie in the flank areas? • The kidneys • What is a common reason for flank pain? • Renal calculi (aka kidney stones)
Kidney Stones • The formation of crystals in the kidney’s collection system • Hospitalization common for pain control and fluid hydration • Additional inpatient treatment may be necessary • Lithotripsy – sound waves used to break apart larger stones into smaller ones that can be passed during urination
Kidney Stones • More common in males • Suggestion of hereditary patterns • Risk factors include immobility and certain medications (anesthetics, opiates, psychotropic drugs) • Stones can form in metabolic disorders (ie: gout) • Production of excessive uric acid and calcium
Stones From Calcium Salts • The most common type of stone • 75 – 85% of all stones • Calcium stones 2 – 3 times more common in men • Average age of onset 20 – 30 years • Familial indication • History of one stone and patient likely to form another one within 2 – 3 years
Struvite Stones • Represent 10 – 15% of all stones • Formation associated with chronic urinary tract infection or frequent bladder catheterization • Patients with spinal cord injuries • Patients with spina bifida • More common in women (due to their higher incidence of UTI’s)
Uric Acid Stones • The least common of all stones • Form more often in men • Tend to occur with family histories so most likely a hereditary component • Half of patients with uric acid stones have gout
Patient Assessment • Chief complaint almost always severe pain • Kidney stones considered to be the most painful medical condition • Pain started vague, dull, poorly localized (visceral pain) in one flank • Within 30 – 60 minutes pain is extremely sharp, remains in the flank and radiates downward and anteriorly to the groin
Physical Exam • Agitated, restless, uncomfortable patient • B/P and heart rate elevated with the pain • Skin typically pale, cool, clammy • Patient may not be able to lie still for abdominal examination • Observed urine sample may have gross hematuria or may be evident only in lab analysis
Management • Position of comfort • Be prepared for vomiting (due to pain) • IV fluids for volume replacement and as a drug route, and to promote urine formation and movement through the system to flush through the stone • Analgesia for pain – limited amounts used in the field often have minimal effect, if at all
Region X SOP - Flank Pain • SOP treatment same as abdominal pain • EMS must call Medical Control to obtain pain medication orders (Region X EMS Morphine 2 mg slow IVP; repeated every 2 minutes to a maximum of 10 mg) • Be patient’s advocate for pain control • Kidney stones are considered the most painful human condition (just ask someone who has had one!)
Hypertensive Emergency • A life-threatening crisis with an acute elevation of the blood pressure • Systolic B/P > 230 mmHg • Diastolic B/P > 120 mmHg • Usually seen in patients with untreated or poorly controlled hypertension
Hypertensive Emergency • Signs and symptoms • Epistaxis – nosebleed • The nasal tissue is very thin and prone to bleed • Headache • “The worst headache in my life” often indicates a subarachnoid bleed • Visual disturbances (ie: blurred, blindness)
Restlessness • Confusion • Nausea and vomiting • Neurologicial changes • Altered mental status to seizures to coma • Complications • Hypertensive encephalopathy • Severe headache, vomiting, visual changes, paralysis, seizures, stupor, coma • Ischemic (clot) or hemorrhagic (bleed) stroke