RENAL SYSTEM
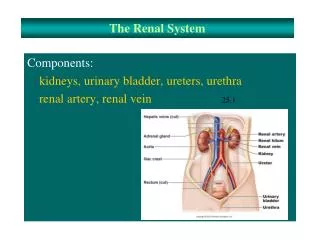
RENAL SYSTEM. Apply principles of pharmacology to safe nursing practice Medications and the renal system. Indications for Diuretic Use. Edema associated with congestive heart failure Acute pulmonary edema Liver disease (including cirrhosis) Renal disease Hypertension

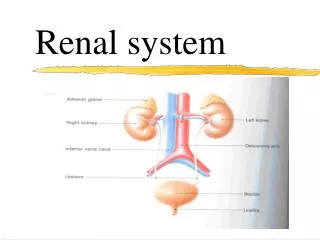
RENAL SYSTEM
E N D
Presentation Transcript
RENAL SYSTEM • Apply principles of pharmacology to safe nursing practice • Medications and the renal system GOTAFE/CSHALDERS2007
Indications for Diuretic Use • Edema associated with congestive heart failure • Acute pulmonary edema • Liver disease (including cirrhosis) • Renal disease • Hypertension • Conditions that cause hyperkalemia GOTAFE/CSHALDERS2007
Sites of Action of Diuretics in the Nephron GOTAFE/CSHALDERS2007
Renal system DIURETICS • Used to remove sodium and water from the body, and for blood pressure reduction • For congestive heart failure • For oedema • For renal impairment, CHRONIC AND ACUTE • Several types of diuretics that work on different parts of the nephron, (functional unit of the kidney) • Thiazide diuretics • Loop diuretics • Potassium – sparing diuretics • Osmotic diuretics GOTAFE/CSHALDERS2007
Indications for Loop Diuretics • Acute CHF • Acute pulmonary edema • Edema associated with CHF • Edema associated with renal or liver disease • Hypertension GOTAFE/CSHALDERS2007
LOOP DIURETICS Potent inhibitors of the reabsorption of sodium and chloride in the thick ascending limb of the Loop of Henle reducing the ability of the kidneys to concentrate urine • Bumetanide (Burinex) • Frusemide (Lasix, Urex) INDICATIONS • Treatment of oedema assoc with heart failure • Cirrhosis • Renal impairment • Nephrotic syndrome • Severe hypocalacemia GOTAFE/CSHALDERS2007
LOOP DIURETICS • They inhibit the reabsorption of chloride and sodium ions from the loop into the interstitial fluid. The result is the interstitial fluid becomes hypotonic. If a high concentration of ions is present water will flow from the collecting duct into the interstitial fluid and back into the bloodstream. • Therefore a hypotonic interstitial fluid will result in diuresis. GOTAFE/CSHALDERS2007
LOOP DIURETICS • Are widely used in current practice, more popular in the elderly with reduced kidney function • Should be used in caution with people with diabetes mellitus, gout, hearing impairment, hepatic and renal impairment. Use in pregnancy should be avoided • More potent than thiazide diuretics • Can lead to K depletion • Can cause hearing loss when used in high doses parenterally GOTAFE/CSHALDERS2007
LOOP DIURETICS • Major problems with loop diuretics are dehydration and electrolyte loss, potasium and sodium main ions affected. • Signs of dehydration should be monitored • Dry mouth • Loss of tissue turgor • Headache and dizziness • Uric acid levels may rise (gout) • Avoid severe nocturnal diuresis GOTAFE/CSHALDERS2007
Frusemide/ Lasix Dose: initially 20-80 mg daily (Max 400mg daily) Adverse effects: fluid and electrolyte disturbances, dehydration, headache, dry mouth blurred vision, dizziness Nursing Implications If starting ACE inhibitor, dose should be decreased for three days prior. Diabetics to monitor BSL more frequently GOTAFE/CSHALDERS2007
Bumetanide /Burinex Dose: 1mg orally daily/ max 10 mg Adverse effects: muscle cramps, fluid and electrolyte imbalance, dizziness, headahe , nausea,hypotension Nursing points: caution if used in those with liver cirrhosis, serum K levels monitored. Interactions: not recommended with lithium Effect of antihypertensive agents may be enhances. GOTAFE/CSHALDERS2007
Ethacrynic/Edecrin Dose: 50-150 mg daily Adverse effects: deafness,vertigo, anorexia, nausea,malaise, blurred vision Interactions: may enhance effect of warfrin, not recommended with lithium, increased risk of gastric heamorrage if given with corticosteroids Nursing points: daily body weight monitoring Dosage may be given on alternate days, stop drugs immediately if watery diarrhoea occurs GOTAFE/CSHALDERS2007
THIAZIDE DIURETICS Act by inhibiting sodium and chloride reabsorption in the ascending loop of henle • Can cause potassium depletion so potassium supplements are often necessary Moderately potent diuretics • Promote renal excretion of water, sodium, chloride potassium and magnesium • Excretion of uric acid and calcium is decreased • Hyperglycaemia has been reported with thiazides GOTAFE/CSHALDERS2007
THIAZIDE DIURETICS • Thiazides have an effect on the peripheral arterioles- which result in vasoldilation • Therefore particularly suitable for hypertensive patients • Thiazides contain sulphonamides should be avoided with known sensitivity • Photosensitivity can occur GOTAFE/CSHALDERS2007
THIAZIDE DIURETICS • Front line treatment for mild to moderate hypertension • Avoid adverse effects by starting with small doses first • Avoid hypokaleamia with potassium replacement GOTAFE/CSHALDERS2007
THIAZIDE DIURETICS • Indapamide (Natrilix) • Amiloride (Midamor) • Chlorothiazide (Clotride) Indications • Mild to moderate hypertension • Oedema associated with heart failure • Cirrhosis with ascites • Prevention of renal calculi GOTAFE/CSHALDERS2007
THIAZIDE DIURETICS • Adverse reactions • Electrolyte imbalance • Dizziness • Weakness • Muscle cramps • Hypotension • Infrequently rash, blurred vision and male impotence • Containdications • In severe renal impairment, anuria and Addisons disease • Rise in blood uric acid levels-problematic those predisposed to gout GOTAFE/CSHALDERS2007
THIAZIDE DIURETICS • Indapamide/ Natrilix • Dose: 2.5mg orally mane or 1.5 mg mane if SR • Adverse effects: fluid and electrolyte imbalance, headache, dizziness, muscle cramps • Interactions: not recommended with other diuretic agents • Nursing points: SR preparations should not be chewed or broken, optimum hypotensive effect is seen in approx 4-6 weeks. GOTAFE/CSHALDERS2007
THIAZIDE DIURETICS • Hydrochlorothiazide/Dithiazide • Dose: 20-100 mg orally 1-2 times daily • Nursing points General for thiazide diuretics GOTAFE/CSHALDERS2007
THIAZIDE DIURETICS • Considered front line for mild to moderate hypertension • Avoid adverse` effects by starting on small dose and gradually titrating according to therapeutic response • High doses more likely to produce adverse effects without approving therapeutic effects • Hypokaleamia less likely to occur if thiazides are administered with and ACE inhibitor GOTAFE/CSHALDERS2007
POTASSIUM SPARING DIURETICS • Advantage they are potassium sparing but not very powerful as diuretics • Two types of potassium sparing diuretics, the aldosterone antagonists and those that act independently of aldosterone GOTAFE/CSHALDERS2007
POTASSIUM SPARING DIURETICS • Aldosterone is the sodium retaining hormone secreted from the adrenal cortex • When aldosterone acts on the distal tubule more sodium ions are retained by the body, water being conserved passively • Is sodium is retained by the nephron at this site potassium is lost • Therefore if aldosterone is blocked potassium is retained and sodium is lost along with a slight increase in diuresis • The phenomenom that induces diuresis, as more ions are lost than retained GOTAFE/CSHALDERS2007
POTASSIUM SPARING DIURETICS • Adverse reactions • Electrolyte disturbances • Nausea • Vomiting • Dizziness • Constipation • Impotence • Headache GOTAFE/CSHALDERS2007
POTASSIUM SPARING DIURETICS • Amiloride • Spironolactone • Triamterene • Limited diuretic efficiancy • Useful when combined with potassium depleting diuretics such as the thiazides • INDICATIONS • For prevention and treatment of diuretic induced hypokalalemia • Adjunct therapy in treatment of odema due to heart failure and hepatic cirrhosis GOTAFE/CSHALDERS2007
POTASSIUM SPARING DIURETICS • Spirolactone/ Aldactone • Dose: 50-100 mg orally • Adverse effects: headache, drowsiness, confusion, nausea • Interactions: may increase serum digoxin, not recommended with other potassium sparing diuretics • Nursing points: taken with food or immediately after, monitor fluid intake, avoid potassium rich foods GOTAFE/CSHALDERS2007
POTASSIUM SPARING DIURETICS • Spirolactone/ Aldactone • Effect of spirolactone is of value when excessive production of spirolactone is involved • Spirolactone very effective in treatment of CCF GOTAFE/CSHALDERS2007
POTASSIUM SPARING DIURETICS • Amiloride/Midamor Act independently of aldosterone • Dose: 10 mg orally daily • Adverse effects: fluid and electrolyte imbalance, hyperkaleamia, nausea and vomiting, thirst • Interactions: not recommended with other potassium sparing diuretics or with lithium • Nursing points: avoid foods high in potassium, electrolyte conc should be monitored GOTAFE/CSHALDERS2007
POTASSIUM SPARING DIURETICS • Most significant adverse effects assoc with these drugs is hyperkalaemia • In men can produce gynaecomastia due to oestrogenic effects • They can induce CNS GIT musculoskeltal dermatological and heamatological adverse effects, most common are nausea and vomiting • Triamterene therapy can induce glucose intolerance which may result in hyperglycaemia GOTAFE/CSHALDERS2007
RENAL SYSTEM DIURETICS – Safe Nursing Practice • Monitoring of fluid balance is essential in early therapy so that dose and effect can be monitored • Monitor blood pressure for effect of medication • Observe for signs of fluid overload or dehydration • Regular serum Potassium levels • Take medication early in the day so that nocturia is not a problem • Watch for signs of electrolyte imbalance such as nausea or vomiting, dry mouth, weakness or lethargy, muscle weakness, cramps. • Some need to be taken with or immediately after food to assist absorption GOTAFE/CSHALDERS2007
Sites of Action of Drugs Acting on the Urinary Tract GOTAFE/CSHALDERS2007
URINARY INCONTINENCE • Before initiating treatment, contributing factors should be eliminated • Urinary tract infections • Excessive fluid intake • High caffeine consumption • Classified into three types • Urge/stress/overflow incontinence • Anticholinergic drugs main group used for urinary incontinence GOTAFE/CSHALDERS2007
DRUGS FOR URINARY INCONTINENCE • Storage and emptying of bladder involves • Integration between central nervous system, spinal cord and peripheral nerves • When bladder full signals sent to brain, internal sphincter relaxes (opens) contraction of detruser muscle and urination occurs • Defects in this pathway leads to incontinence or urinary retention GOTAFE/CSHALDERS2007
ANTICHOLINERGICS • Acetylcholine is the neurotransmitter that controls the detruser muscle • Over activity of this muscle leads to urge incontinence • Drugs that block acetycholine can control urge incontinence • Oxybutynin • Propantheline • Tolterodine Adverse reactions • Dry mouth • Blurred vision • Constipation • Urinary hesitancy GOTAFE/CSHALDERS2007
Patient Education to Avoid a UTI • Avoid foods that cause an alkaline ash and produce an alkaline urine (e.g., citrus juices, fruits, antacids) • Drink high-acid cranberry juice • Void immediately after sexual intercourse • Avoid baths if possible, especially bubble baths (women) • Wipe front to back and never back to front (women) GOTAFE/CSHALDERS2007
Signs and Symptoms of a UTI • Urinary frequency • Urgency • Burning on urination (associated with cystitis) • Chills, fever, flank pain, and tenderness (associated with acute pyelonephritis) GOTAFE/CSHALDERS2007
Treatment for UTIs • Antibiotics • Specific agents to sterilize the urinary tract • Drugs that: • Block spasms of the urinary tract muscles • Decrease urinary tract pain • Protect the cells of the bladder from irritation • Treat enlargement of the prostate gland in men GOTAFE/CSHALDERS2007
Osmotic Diuretics • Directly interfere with osmosis • Any substance that that enters the body in large quantities and is excreted via the kidneys will lead to water being kept in the renal tubules, leading to water loss • Given parenterally produce fast diuresis in emergency situations • Should be non toxic, be excreted quickly, and not be reabsorbed by the glumerular filtrate • They therefore must be water soluble, must be given intravenously GOTAFE/CSHALDERS2007
Osmotic Diuretics • Types • Glycerin (Osmoglyn), Isosorbide (Ismotic), Mannitol (Osmitrol), and Urea (Ureaphil) • Action • Pull water into the renal tubule without sodium loss effective in increasing osmotic pressure • Indications • Increased cranial pressure or acute renal failure due to shock, drug overdose, or trauma GOTAFE/CSHALDERS2007
Osmotic Diuretics • Osmotic diuretics tend to remain in the blood and by increasing the osmolarity of the blood are useful in the treatment of oedematous states • The fluid from oedematous states is extracellular and will therefore pass from these areas into the hypertonic blood, and then to the kidneys for removal GOTAFE/CSHALDERS2007
Osmotic diuretics • Adverse effects • Electrolyte imbalance and potential for dehydration • Can result in hypervolaemia • Mannitol infusion bag crystallises at low temperatures GOTAFE/CSHALDERS2007
Urinary Alkalinisers • Raise PH of urine • Pain in urinary tract infections is due to the high acicidity of urine burning the urethra • E coli does not grow well at high PH GOTAFE/CSHALDERS2007
Urinary Alkalinisers • Used to help treat urinary tract infections • Examples:- • Sodium citrotartrate (Ural) • Citravescent sachets • Nursing implications • Ensure the infection is being treated not just the symptoms • Not recommended for people with heart failure or low urine output GOTAFE/CSHALDERS2007
Urinary Alkalinisers • Alkalinisation of urine is useful to relieve the painful dysuria in cystitis. • Most of the pain is caused by high acidity burning the urethra • Escherichia coli organism does not grow well at high Ph levels • In case of poisoning with acidic drugs such as asprin, alkalinisation of the urine will increase the excretion of the drug GOTAFE/CSHALDERS2007
Urinary Alkalinisers • Clinical considerations • Alkalinisation is possible only if creatinine clearance is at least 30ml/min • May be necessary to check clients renal function before administration GOTAFE/CSHALDERS2007
Client Teaching • Be aware of potassium supplements • Clients with diabetes to monitor BSL as thiazides and potassium sparing can cause hyperglycaemia • Teach manifestations of hypocalcaemia: muscle cramps weakness and lethargy • Manifestations of hyperkaleamia: thirst dry mouth and drowsiness • Avoid alcohol can enhance hypotension caused by diuretics • Watch postural hypotension GOTAFE/CSHALDERS2007
References Marieb, E. 2006, Essentials of Human Anatomy & Physiology, 8th edition, Pearson, Benjamin, Cummings. USA Herlihy, B. 2007 , The Human Body in Health and Illness, 3rd edition, Saunders Elsevier. St Louis, USA Thibodeau, G. Patton, K. 2002, The Human Body in Health & Disease, 3rd edition, Mosby. St Louis, USA Cohen, B. Taylor, J. 2005, Memmler's Structure and Function of the Human Body, 8th edition, Lippincott,Williams & Wilkins. USA Anatomy & Physiology made Incredibly Easy, 2000. Springhouse. Pennsylvania, USA Anatomica, 2000, Random House Australia Pty Ltd GOTAFE/CSHALDERS2007 46