Download
1 / 1
10 likes | 143 Views
Poster 796 15th Conference on Retroviruses and Opportunistic Infections 3-6 February 2008 - Boston, USA. S Arponen, JM Benito Hospital Carlos III C Sinesio Delgado 10 – 28029 Madrid (Spain) arponen@gmail.com +34915232531.

E N D
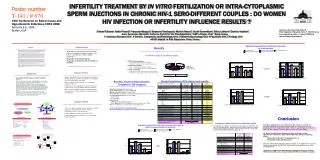
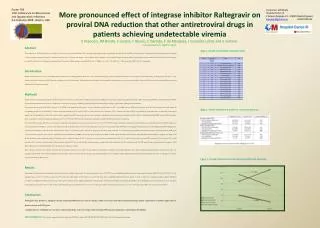
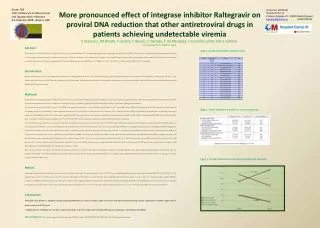
Poster 796 15th Conference on Retroviruses and Opportunistic Infections 3-6 February 2008 - Boston, USA S Arponen, JM Benito Hospital Carlos III C Sinesio Delgado 10 – 28029 Madrid (Spain) arponen@gmail.com +34915232531 More pronounced effect of integrase inhibitor Raltegravir on proviral DNA reduction that other antiretroviral drugs in patients achieving undetectable viremia S Arponen, JM Benito, S Lozano, F Blanco, C Garrido, C de Mendoza, J González-Lahoz and V Soriano. Hospital Carlos III, Madrid, Spain. Abstract The eradication of HIV infection from the resting T-cell reservoir is an unsolved challenge. The new antiretroviral drugs may play a promising role in this aim. ProviralDNA was measured in 10 antiretroviral-experienced patients who initiated a salvage regimen containing raltegravir. A matched control group of 8 patients who begun a rescue regimen without raltegravir was examined. Despite all patients achieved undetectable plasma viremia during the first 12 weeks of therapy, proviral DNA declined in 8/10 patients on raltegravir and 3/8 controls. Median changes in proviral DNA were -41 (IQR, -16 to -63) vs +51 (IQR, -4 to +149) copies/µg of DNA (p=0.03), respectively. Introduction Despite HAART permits to reach undetectable plasma viremia in most adherent patients, HIV can not be eradicated. Integration of the viral genetic material into some long-life cells precludes this goal. Raltegravir is the first of a new antiretroviral family which prevents HIV genome to integrate into host chromosomes. We hypothesize that throughout this mechanism it might produce a more pronounced decline in proviral DNA than other antiretroviral drugs, even after adjusting for viral response in plasma. Methods Heavily antiretroviral experienced patients with HIV resistant to at least the 3 classical antiretroviral drug classes initiated Raltegravir along with an optimized background therapy. CD4 counts, plasma HIV-RNA and proviral DNA in PBMC were measured at baseline and at week 12 of treatment. A matched control group of multidrug-resistant patients who similarly begun a salvage regimen without Raltegravir was evaluated. For quantification of proviral HIV-DNA, aliquots of 106 PBMC were obtained at each patient´s visit and cell pellets stored frozen at –60ºC. A modified real time PCR method was then used. DNA was extracted from cell samples by resuspending the pellet in 100 microliters of a buffer containing proteinase K at 100 μg/ml at 56ºC for 2 hours and then for 15 minutes at 95ºC to inactivate the enzyme. DNA was quantified by spectrophotometry to determine its amount per sample. The T lymphoblastoid cell line 8E5, which contains a single proviral HIV genome per cell, was used to generate a standard curve by performing serial log dilutions. 8E5 cells were serially diluted with PBMC from an HIV-seronegative donor to generate five different standards containing from 106 to 102 8E5 cells. DNA from the standards was extracted in parallel with DNA from patient´s specimens. For real-time PCR, the input DNA from the standards was calculated and experiments were done using from 5 X 104 to 5 X 101 HIV-DNA copies. For patient´s specimens, the DNA input was 1 μg. The total volume of the PCR mixture was 20 μl and contained 4 mM MgCl2, 0.5 μM of each primer, 0.25 μM of specific probes, 0.5 U of Uracil D-glycosilase, and 10 μl of the Quantitec Probe PCR Master Mix (Qiagen). Primer sequences used for amplifying the HIV-LTR gene were: forward primer, LTR152 (5´-GCC TCA ATA AAG CTT GCC TTG A-3´); and reverse primer, LTR 131 (5´-GGC GCC ACT GCT AGA GAT TTT-3´). The specific probe was labeled with the reporter dye 6-carboxy fluorescein (FAM) at the 5´end, and with the quencher dye N,N,N´,N´-tetramethyl-6-carboxy-rhodamine (TAMRA) at the 3´end, and its sequence was: LTR1 (5´-FAM-AAG TAG TGT GTG CCC GTC TGT TRT KTG ACT-TAMRA-3´) (Qiagen). The Light-Cycler (Roche Molecular Systems, Barcelona, Spain) PCR protocol was as follows: 2 minutes at 50ºC (1 cycle) for carryover prevention, denaturation at 95ºC for 15 minutes (1 cycle); and a two-step PCR consisting of 10 seconds at 95ºC and 60 seconds at 60ºC (45 cycles). For data analysis with the channel setting F1/F2, the second derivative maximum mode was used with baseline adjustment set in the arithmetic mode. The HIV prrovial load was expressed as the number of HIV-DNA copies per μg of total cellular DNA, with a threshold of 5 copies/μg of DNA. Drug resistance mutations were assessed at baseline and the genotypic sensitivity score (GSS) was determined for each subject according to the Stanford algorithm v4.3.1 (http://hivdb.stanford.edu/pages/asi/releaseNotes/). Data were analyzed using the SPSS v15.0 software. Differences between median values in both groups were assessed using the Mann Whitney U test. Changes in plasma HIV-RNA, CD4 cell counts and proviral load at week 12 with respect to baseline were assessed using the Wilcoxon test. Results Both groups had similar baseline demographic, clinical, and immuno-virologic characteristics. The genotypic sensivity scores of HAART were not significantly different between both groups (the median (IQR) GSS was 2.25 (1.88-2.25) in the raltegravir group and 2.3 (1.81-2.94) in controls (p=0.70)). The mean (SD) length of HIV infection was 14.8 (4.4) years, with no significant differences between groups. At week 12, there was a significant decline in plasma HIV-RNA (p<0.0005) and CD4 gain (p<0.001) in both groups with respect to baseline, without significant differences between groups. However, proviral DNA load declined significantly only in the Raltegravir arm. It decreased in 8 out of 10 patients treated with raltegravir and 3 out of 8 controls. The median (IQR) change in proviral DNA was -41 (-16 to -63) copies/µg of DNA in the raltegravir group, and +51 (-4 to +149) copies/µg of DNA was seen in controls (p=0.03). Conclusions -Raltegravirmay produce a significant decline in proviral DNA after 12 weeks of therapy, which is not seen with other antiretroviral drugs despite achievement of similar suppression of plasma viremia and CD4 gains. -A higher potency of Raltegravir over other antiretroviral drugs and/or its unique effect blocking HIV genome integration could explain this finding. Acknowledgment: This work was supported in part by grants from FIPSE, Fundación IES, FIS (ISCIII-RETIC RD06/006), NEAT and AgenciaLaínEntralgo. Table 1. HAART and Genotypic Sensitivity Score. Table 2. Results at baseline and week 12 compared by groups. Figure 1. Change of plasma viral load and proviral DNA load by groups. P = 0.83