GIT.3 Dr. Basim
Explore the anatomy of the stomach, congenital anomalies like pyloric stenosis, and chronic conditions such as gastritis. Learn about the etiology, pathogenesis, morphology, and clinical features of acute and chronic gastric conditions.

GIT.3 Dr. Basim
E N D
Presentation Transcript
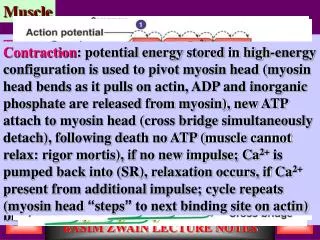
Pathology of Stomach: Histology of stomach: • Mucosa: Composed of gastric pits (foveolae), & gastric glands. • Glands are either: • MUCUS SECRETING GLANDS at the antrum & cardia. • Acid- pepsin secreting glands (chief cells secrete pepsin, parietal cell secrete HCL & intrinsic factor). • Other layers (submucosa, muscularis layer, serosa).
Congenital anomalies: 1. Pyloric stenosis: • First male baby, • muscular hypertrophy of pyloric sphincter. • Important feature is projectile vomiting in early infancy 2. Gastric hetrotopia: • Uncommon, clusters of gastric mucosa in the esophagus or small intestine……. Peptic ulcer in ectopic site. • Gastritis: inflammation of gastric mucosa. • Either acute or chronic Acute gastritis: • Acute mucosal inflammatory process usually of a transient nature. Etiology: • Heavy use of non steroidal ant inflammatory drugs (aspirin). • Excessive alcohol consumption. • Heavy smoking. • Uremia. • Systemic infection (salmonellosis). • Severe trauma (burn, trauma, surgery).treatment with anticancer drugs. • After distal gastrectomy. • Mechanical trauma (nasogastric tube).
Pathogenesis: Acute gastritis is due to followings: • Disruption of adherent mucous layer. • Stimulation of acid secretion with hydrogen ion diffusion into superficial epithelium. • Decreased production of bicarbonate buffer by superficial epithelial cells. • Reduced blood flow of mucoasa. • Direct damage to epithelial cells. • Acute infection by H. pylori. Morphology: • From Localized acute gastritis…… associated with NSAID to diffuse type. • From superficial acute inflammation……. To full thickness inflammation with hemorrhage & focal erosion (acute erosive gastritis). • Mic: mucosal edema + neutrophils infiltration +erosion + regeneration of surface epithelial cells. • Clinical features: • Epigastric pain, nausea & vomiting, hematemesis (in alcoholic).
Chronic gastritis: Is defined as presence of chronic mucosal inflammatory changes leading eventually to mucosal atrophy & epithelial metaplasia. Sometimes cause dysplasia, which predispose to carcinoma. • There is no erosion (to differentiate from gastric ulceration). Etiology: • Chronic inflammation (by H.pylorii)……. Present in 90% of cases. • Autoimmune cause (pernicious anemia)…. Autoantibodies in 10% of cases. • Toxic e.g. alcohol, cigarettes smoking. • Post surgical e.g. biliary reflux after gastric surgery. • Radiation • Granulomatous inflammation e.g. T.B. • Motor & mechanical causes (obstruction & bezaors). Classification: • Type "A" chronic gastritis. • Type "B" chronic gastritis.
Type A Chronic gastritis: • Autoimmune gastritis. • Associated with other autoimmune diseases e.g. D.M. • Occur in adult life. • Mostly in the fundal area. • There are autoantibodies against parietal cells which result in followings: • Decreased HCL production • Decreased production of INTRINSIC FACTOR….. impaired B12 absorption….. pernicious anemia. • High risk of developing Gastric carcinoma. Mic:three stages • Chronic superficial gastritis: inflammatory infiltrate into the foveolar part of epithelium (mainly lymphocytes & plasma cells). • Chronic atrophic gastritis: inflammation involves foveolar & deeper part of mucosa….. Glandular destruction & loss, decreased in mucosal thickness, & intestinal metaplasia (goblet cells). • Gastric atrophy: • Thinning of mucosa. • Minimal inflammatory infiltrate within lamina properia.
Clinical features: • Epigastric pain, pernicious anemia. Type "B" chronic gastritis: • Also called environmental type. • More common than Type A. • At any age. • Mainly at antrum. • Main causative agent is H. pylori (80% of cases). • Less common causes (chronic alcohol abuse, cigarettes, NSAID). • Highly associated with GASTRIC ULCER , BUT less associated with gastric carcinoma than Type A. Mic: • Inflammatory infiltrate (lymphocytes, plasma cells & neutrophils in active cases). • Some Glandular atrophy & intestinal metaplasia.
Acute gastric ulceration: • Is means development of focal, acutely developing mucosal defects. Causes: • Severe trauma (major surgical procedures, sepsis). • Extensive burns (Curling ulcer). • Traumatic or surgical injury to the central nervous system or an intracranial hemorrhage (Cushing ulcer). • Chronic exposure to NSAID.
Pathogenesis: • Acute ulcer can occur due to followings: • Chronic NSAID use……. Decrease PG secretion……. Mucosal ulcer. • Stress impairs blood supply to mucosa….. decrease oxygenation of mucosa……. Mucosal sloughing. • Head trauma…..vagal stimulation…….. increase HCL secretion…… ulceration • Systemic acidosis due to trauma……….. affect bicarbonate buffer of mucosal cells………… mucosal ulcer. Mic: Multiple, small (less than 1cm), oval- round, variable in thickness (from superficial erosion to full thickness gastric ulcer)…. Sometime perforation.
Clinical features: • Features of underlying condition (head injury, drugs abuse) + UPPER GASTROINTESTINAL BLEEDING. Chronic gastric ulcer: • Ulcer: is a defect in the mucosa causing a discontinuity of the surface epithelium which may extend into the muscularis mucosae into the submucosa, or deeper. • Peptic ulcer: is an ulcer occur in the areas of the GIT that are exposed to the acid – pepsin secretion as in: (sites) 1. Duodenum 2. Stomach (both 1,2 form 98% of cases). 3. Lower esophagus (Barrett esophagus). 4. Margin of gastroenterostomy (stomal ulcer). 5. at meckle's diverticulum that contain foci of gastric tissue.
Epidemiology: • The ratio of duodenal ulcer/gastric ulcer = 4/1 • Male /Female = 3/1 for duodenal ulcer, 2/1 for gastric ulcer. • Racial & genetic factors have no role in the causation of peptic ulcer. • It is characterized by remission & relapse. • D.U is more frequent with alcoholic liver cirrhosis, chronic obstructive airways diseases, chronic renal failure & hyperthyroidism. Pathogenesis: • Peptic ulcer appears to be produced by an imbalance between the gastroduodenal defense forces & Aggressive forces (damaging forces). Defense forces: • Surface mucous layer secreted by epithelial cells. • Bicarbonate secretion into the mucous. (buffer of mucosa) • Secretion of acid – pepsin containing fluid as "jets" into the lumen without contact the surface epithelium. • Rapid gastric epithelial regeneration.
5. Rapid mucosal blood flow to remove away Hydrogen ions that enter the mucosa from lumen. 6. Mucosal elaboration of PG….. maintain the blood flow. Aggressive forces: • Hyperacidity (high HCL secretion)……. Associated with few cases of D.U, not with G.U. • Peptic enzymes (pepsinogen). • Others: ……. H. pylori ……… NSAID (aspirin) ……… Cigarettes smoking ……… Alcohol
The most important cause is H.pylori infection, by following evidences. • 70% - 90% of D.U are positive for H.pylori. • 70% of G.U are positive for H.pylori. • Antibiotic treatment for H.pylori infection promotes healing of ulcers & prevents recurrence. H. pylori causes peptic ulcer by following mechanisms: 1. Non invasive bacteria induce inflammation by increased production of inflammatory mediators from mucosal cells. 2. H.pyloriinduce epithelial cell injury & inflammation by production of: iurease…. Breakdown of urea into toxic metabolites……. Mucosal cell injury. ii. Phospholipase & proteases………. Damage the surface epithelial cells. 3. Impaired bicarbonate production by increase production of HCL from parietal cells……..induce gastric metaplasia in first part of duodenum. 4. induces both T cells & B cells proliferation ……..may play role in pathogenesis of gastric lymphoma.