Download
1 / 18
240 likes | 845 Views
Polycystic Ovarian Syndrome (PCOS). Elaine Sunderlin, MD – PGY-2 Morning Report September 15, 2009. Background . First described in 1935 by Stein and Leventhal Affects 5-10% of women of reproductive age making it the most common endocrine disorder is this age group

E N D
Polycystic Ovarian Syndrome(PCOS) Elaine Sunderlin, MD – PGY-2 Morning Report September 15, 2009
Background • First described in 1935 by Stein and Leventhal • Affects 5-10% of women of reproductive age making it the most common endocrine disorder is this age group • Characterized by oligomenorrhea, amenorrhea, infertility and hirsutism. Occasionally associated with enlarged ovaries
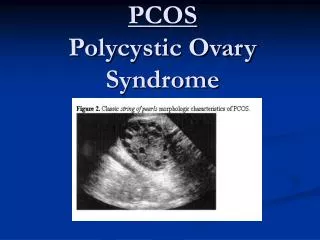
Diagnostic Criteria - ACOG • Major • Chronic anovulation • Clinical signs of androgen excess (hirsutism, acne, alopecia, mentrual disturbance, infertility, virilization • Exclusion of alternative causes of androgen excess • Minor • Insulin resistance • Onset at puberty • Elevated LH:FSH (>2.5-3) • Ultrasound evidence of polycystic ovaries
Diagnostic Criteria - Rotterdam • Oligo- or anovulation • Clinical and/or biochemical signs of hyperandrogenism • Polycystic ovaries • 2 out of 3 required for diagnosis
Menstrual irregularities • Amenorrhea: up to 10% of patients present with primary amenorrhea and 75% present with secondary amenorrhea • May have intermittently regular and fertile cycles despite elevated androgen levels • If pregnancy does occur, there is increased risk of gestational diabetes and pregnancy-induced HTN
Hyperandrogenism • Pts w/ PCOS have an increased sensitivity to androgens; up to 70% have elevated androgen levels and the other 30% are in the high-normal range • 3 major circulating androgens: • Androstenedione (>90% produced in ovaries, produced by ovarian stromal and thecal cells in response to LH. Normally converted to estradiol by FSH dependent aromatase) • DHEA-S (mainly produced in adrenals) • Testosterone (produced in ovaries and adrenals in equal amounts)
Clinical signs of Hyperandrogenism • Hirsutism: excessive growth of terminal, pigmented hair on androgen sensitive areas (chin, upper lip, sideburns, sternal, periareolar, umbilical and sacral areas) with accentuated involvement of the pubic region and upper thighs • Alopecia is much rarer manifestation of PCOS • Acne: severe cystic and persistent acne is usually androgen-dependent • Virilization usually mild. If more severe signs (clitormegaly, deepening of the voice & incr muscle mass) are present, underlying diseases of adrenal and pituitary glands (CAH, hyperprolactinemia, or androgen-secreting tumors) need to be excluded • Hyperandrogenic effects usually progress slowly
Metabolic derangements • Insulin resistance with increased risk of development of type 2 DM • Hyperinsulinemia • Increased risk for development of metabolic syndrome • Obesity, especially central visceral obesity, is present in 35-80% of patients
Hyperandrogenism causes hyperinsulinemia or vice versa? • Decreasing androgen levels does not reduce hyperinsulinemia in PCOS • Induced hyperandrogenism in females w/o PCOS does not alter insulin sensitivity • Insulin resistance persists after oophorectomy or after ovarian androgen synthesis is suppressed by GnRH agonists
Hyperandrogenism causes hyperinsulinemia or vice versa? • Giving insulin to PCOS patients increases circulating androgen levels and lowering insulin by using diazoxide lowers androgen levels • Insulin stimulates androgen production in ovarian thecal cells in PCOS • Insulin amplifies the LH response of granulosa cells, thereby causing an abnormal differentiation of these cells, premature arrest of follicular growth, and so anovulation
Pathophysiology • Exact pathophysiology or initiating event are unknown
HPG Axis abnormalities • Elevated LH w/ low to nml FSH • In PCOS, normal pulsatile secretion of LH is increased by an increased frequency and amplitude of pulses while FSH is unchanged or muted • Elevated prolactin • Levels are increased in ~25% of pts. Extreme elevations may stimulate adrenal production of dihydroepiandrosterone sulfate (DHEA-S)
HPG Axis abnormalities • Increased GnRH: inappropriate secretion of gonadotropins thought to be due to abnormality of GnRH pulse generation in hypothalamus • Primary: study of girls w/ fmhx who were entering puberty showed LH pulses in late afternoon (nml is at night) • Secondary: females develop a PCOS-like condition in Cushings, exposure to anabolic steroids, or w/ androgen-producing tumors.
Long-term Consequences • Increased risk of endometrial cancer due to the unopposed effect of estrogen on the endometrium • Tonic and abnormal stimulation of the ovaries felt to be related to elevated risk of ovarian cancer • Type 2 DM • CAD
Treatment • Diet, exercise and weight loss • Studies have shown that androgen production is significantly decreased with a little as 10-15 lbs loss over 6 months • Oral contraceptives • Antiandrogens (spironolactone) • Insulin sensitizers • GnRH agonists
OCPs • Establish regular menstrual cycles • Reduce gonadrotropin stimulation of ovaries, thus reducing androgen production • Increase SHBG • Inhibit androgen receptor binding • Use newer progestins (desogestrel, norgestimate) because of minimal androgen effects
Spironolactone • Blocks androgen receptor from “seeing” dihydrotestosterone. May also suppress androgen biosynthesis • 40-80% reduction in sexual hair growth • Requires 8-14 months before clinical effects can be seen • Use in combination with OCPs as it has minimal effect on free testosterone and androstenedione. Also can cause polymenorrhea due to the effect on the endometrium
References • Marx, Theresa and Adi Mehta, MD. Polycystic Ovarian Syndrome: Pathogenesis and treatment over the short and long term. Cleveland Clinic Journal of Medicine. Vol 70, No. 1, January 2003. 31-41. • Franks, Stephen. Diagnosis of Polycystic Ovarian Syndrome: In Defense of the Rotterdam Criteria. Journal of Clinical Endocrinology & Metabolism. 91(3):786-789