Download

1 / 19
290 likes | 921 Views
Polycystic Ovary Syndrome. Krishna B. Singh, MD Department of Obstetrics & Gynecology LSU Health Sciences Center Shreveport, LA. PCOS: Learning Objectives. After viewing this slide show, you’ll be able to understand that... -PCOS is a common endocrine disorder

E N D
Polycystic Ovary Syndrome Krishna B. Singh, MD Department of Obstetrics & Gynecology LSU Health Sciences Center Shreveport, LA
PCOS: Learning Objectives After viewing this slide show, you’ll be able to understand that... -PCOS is a common endocrine disorder -Multifactorial, heterogeneous condition -Clinical manifestations affect menses, fertility -Multiple hormonal, biochemical changes -Long-term implications are important
PCO Syndrome: Topics • Historical review • Incidence • Clinical features • Diagnosis • Management • Summary
PCOS: Literature Review • Sclerocystic ovaries were described by Chereau (1844); Pozzi (1894); Waldo (1895) • Stein/Leventhal first described seven cases of infertility associated with enlarged polycystic ovaries (1935) • The NIH Consensus Conference (1990) • The Rotterdam PCOS Consensus Group (2003)
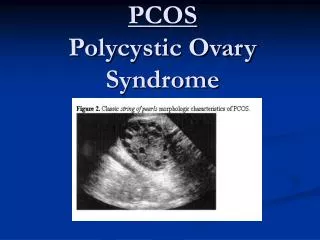
Incidence: PCO Syndrome • The incidence varies: 5-10% (~5% USA) • About 25% normal women may have PCO by ultrasound criteria (BMJ 1986) • Ultrasound findings don’t correlate with serum hormone levels
Features of PCO Syndrome • Symptoms present since puberty: Cyclic menses with luteal-phase progesterone deficiency; hirsutism; hyperandrogenemia; infertility; chronic anovulation/miscarriages • Irregular menses in 25-75% women • Obesity (60%); also non-obese women • Hirsutism and/or acne (virilization rare)
Polycystic Ovarian Disease • PCO disease can be seen in women with pituitary neoplasms, hypo- or hyperthyroidism, diabetes, adrenal and pelvic neoplasms • Rule out PCOD to diagnose PCO syndrome • Long-term care is important. Studies have shown increased incidence of hypertension, hyperlipidemia and diabetes. Risk for CVD increased
PCO Syndrome: Facts/correlates • Genetic factors: autosomal or X-linked • Positivecorrelations of androgen and insulin levels in some studies • Ultrasound findings don’t correlate with serum hormone levels
Theories of PCO Syndrome • PCO syndrome is a multifactorial disorder • Theories are based on data in selectedwomen • Brain and limbic system control the hypothalamus-pituitary-ovarian axis needed for reproductive cycle initiation and maintenance • Feedback CNS abnormality results in PCOS
CNS theories of PCO • Beta-endorphin theory:Higherplasma levels are found in women with PCO syndrome • Progesterone deficiency/estrogen excess is the key component • Hyperandrogenism also important in PCO women • Hyperprolactinemiamay cause breast symptoms, diminish libido, and alter moods in some women
More PCO Theories... • Rat PCO model: Persistent-estrus syndrome • Constant-light exposure; androgenized rat model; hypothalamic lesions • Other methods (DHEAS model) • Monkey model: testosterone injections • Human model: transvestites given androgens
Diagnosis of PCO Syndrome • History and physical examination important; selected laboratory and hormonal tests during several visits are needed for confirmation • Both structured and descriptive notes are evaluated by the physician • Follow-up visits arranged @ regular intervals
PCOS: Differential Diagnosis • Laboratory tests for confirmation: LH/FSH, T • Baseline values: Chem-22 @ morning • Baseline serum hormones @ morning • Pelvic ultrasound in some cases required • Consider PCOD versus PCO syndrome
PCOS: Key to Diagnosis • Rule out conditions which may require referral;focus on the presenting signs and symptoms • Beware of misdiagnosis “on the fly” • Beware of differential diagnosis • History and physical exam; selected tests • Know when to refer patients and where
PCOS: Management Options • Principal components:Confirm diagnosis and identify category; identify and manage concurrent illness; identify and manage patient needs • There are numerous options for successful PCO management
PCOS: Treatment Options • General measures:diet, exercise, relaxation for stress management • Contraception: OCP; DMPA • Hormones/drugs:Provera; Parlodel; Clomiphene; hMG/hCG; IVF in selected women • Newer drugs for treatment of obesity, hyperinsulinemia, hyperandogenemia and hirsutism
PCO Syndrome and Infertility • About 60% PCO patients will have ovulatory cycles and pregnancy on clomiphene alone • About 50% PCOpatients will respond to the combined clomiphene and dexamethasone within six months of treatment
PCO Syndrome: Summary • PCO syndrome remains an enigma despite many scientific studies done during the last three decades • Theories of PCO abound; terminology used may be confusing and definitions are not standardized • There are many treatment options
What This Means... • Polycystic ovary syndrome is a common disorder among reproductive age groupof women; these women generally have irregular menstrual cycles • PCO has many facets of clinical presentation • PCO can be successfully managed and treated by conventional means