Download
1 / 84
1.18k likes | 2.65k Views
POLYCYSTIC OVARY SYNDROME (PCOS). Yasser Orief M.D. Fellow , Lübeck University, Germany. DAOG, Auvergné University, France. Agenda. Definition Epidemiology Pathophysiology Diagnostic approach Long term Consequences Treatment Follow up. PCOS: History. 1721 Antonio Vallisneri

E N D
POLYCYSTIC OVARY SYNDROME (PCOS) Yasser Orief M.D. Fellow , Lübeck University, Germany. DAOG, Auvergné University, France.
Agenda Definition Epidemiology Pathophysiology Diagnostic approach Long term Consequences Treatment Follow up
PCOS: History • 1721 • Antonio Vallisneri • “…Young peasant woman, married, moderately plump, infertile, with ovaries larger than normal, like doves’ eggs, lumpy, shiny and whitish” • 1935 • Dr. Irving Stein and Dr. Michael Leventhal • Coined Stein-Leventhal disorder • 1980 • Linked to hyperinsulinemia and impaired glucose tolerance • 2006 • What causes PCOS? Lanham 2006
Stein and Leventhal They were the first to recognize an association between the presence of polycystic ovaries and signs of hirsutism amenorrhea (oligomenorrhea, obesity) Polycystic Ovarian Disease After successful wedge resection of the ovaries in women diagnosed with Stein-Leventhal syndrome, menstrual cycles become regular and the patients were able to conceive. Primary ovarian disorder come to be known as polycystic ovarian disease Polycystic ovarian syndrome Biochemical, clinical and endocrinological abnormalities have shown an array of underlying abnormalities; hence condition known as polycystic ovarian syndrome( PCOS) Syndrome O gets to the real heart of the problem and indicates: Ovarian confusion and Ovulation disruption caused primarily by Over nourishment and Overproduction of insulin In reality PCOS, infertility, and other health problems may be all consequences of syndrome O Introduction
Introduction • Most attention has been paid to the management of the presenting complaint (infertility, hirsutism.. etc.) • It has become clear that the polycystic ovary phenotype is linked to a number of metabolic disturbances, including type II diabetes and possibly atherosclerosis • Since PCOS frequently diagnosed by gynecologists, it is therefore, important that gynecologists have a good understanding of the long-term implications of the diagnosis
Common names and confused with… • Stein-Leventhal Syndrome • Polycystic ovary disease • Functional ovarian hyperandrogenism • Hyperandrogenic chronic anovulation • Ovarian dysmetabolic syndrome • Polycystic ovarian syndrome
Definition Stein and Levanthal (1935): association of amenorrhea with polycystic ovaries and variably: hirsutism and/or obesity ACOG and NIH (1990): hyperandrogenism and chronic anovulation excluding other causes
Criteria of the PCONational Institutes of Health • Presence of menstrual abnormalities and anovulation • Presence of clinical and/or biochemical hyperandrogenaemia • Ultrasound examination ? • peripheral cysts (10 or more) less than 10mm in size in an enlarged ovary with significant increase in the central stroma • Absence of hyperprolactinaemia or thyroid disease • Absence of late-onset congenital adrenal hyperplasia • Absence of Cushing’s syndrome
2003 ESHRE/ASRM-sponsored PCOS Consensus workshop • 1990 Criteria (both 1 and 2) • 1. Chronic anovulation and • 2. Clinical and/or biochemical signs of hyperandrogenism • and exclusion of other etiologies. • Revised 2003 criteria (2 out of 3) • 1. Oligo- or anovulation • 2. Clinical and/or biochemical signs of hyperandrogenism, • 3. Polycystic ovaries and exclusion of other causes of hyperandrogenism (congenital adrenal hyperplasia, androgen-secreting tumors, Cushing's syndrome)
PCOS: Diagnostic Criteria • Other concurrent manifestations • Insulin resistance • Features of metabolic syndrome • Increased risk for diabetes mellitus II, cardiovascular disease, endometrial bleeding or cancer Milnar et al. 2006 Carmina 2006
Appearance of ovaries • Polycystic ovaries are enlarged bilaterally and have a smooth thickened capsule that is avascular • On cut section, subcapsular follicles in various stages of atresia are seen in the peripheral part of the ovary • The most striking ovarian features of PCOS is hyperplasia of the theca stromal cells surrounding arrested follicles • Microscopically luteinizing theca cells are seen
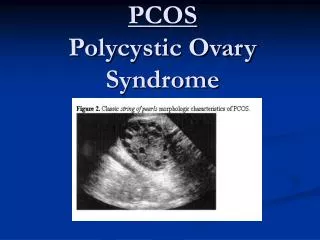
increased size and a smooth white surface reflecting thickening of the capsule
Showing multiple cysts with diameter <10mm arranged around the periphery of the ovary. The stroma is increased, and the ovary enlarged
Epidemiology • Prevalence: 4-6% females • Probably same world wide • No difference between blacks and whites • 75% of women w/ irregularity or infertility
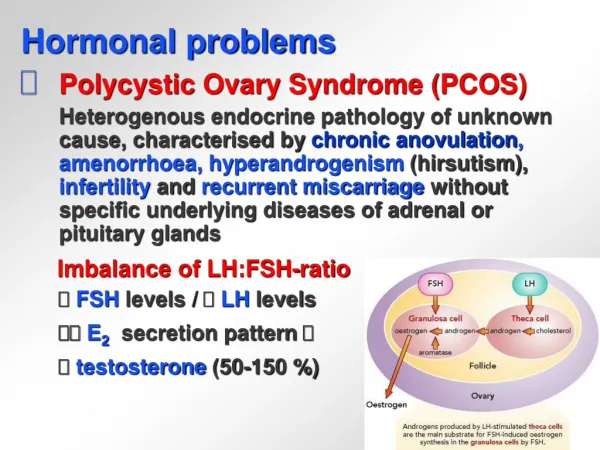
PCOS: PathopysiologyWhat we think we know. • “Vicious cycle” • Abnormal gonadotropin secretion • Excess LH and low, tonic FSH • Hypersecretion of androgens • Disrupts follicle maturation • Substrate for peripheral aromatization • Negative feedback on pituitary • Decreased FSH secreation • Insulin resistance, Elevated insulin levels
PCOS: Current theories of pathopysiology Autosomal Dominant Gene Downstream Signal Defect GnRH E2 LH Insulin Resistance PCOS A A=androgens, E2=estradiol
Theories of the Pathogenesis of PCOS Salehi M. et al., Metabolism 2004; 53: 358-376
PATHWAYS LEADING TO ANDROGEN EXCESS IN PCOS Tscichorozidou T et al.., Clin Endocrinol 60: 1-17, 2004
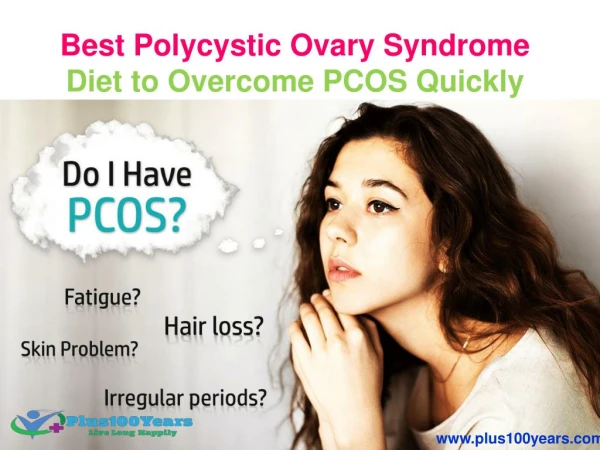
SYMPTOMS Menstrual irregularity Infertility Hirsutism, acne, etc Obesity SIGNS Hirsutism, acne Obesity Ovarian enlargement Acanthosisnigricans PCOS: Signs and Symptoms
Polycystic Ovarian Syndrome • History • Complete a good menstrual history • menarche • duration, frequency, intensity of bleeding • periods always irregular or new onset • Menorrhagia / metrorrhagia • Attempt to determine if irregular bleeding ovulatory or anovulatory
Polycystic Ovarian Syndrome • History • Ovulatory bleeding suggested by presence of premenstrual symptoms: • breast engorgement • pelvic cramping • fluid retention • mood swings • Menstrual regularity more suggestive of ovulatory • Anovulatory • absence of premenstrual symptoms • frequently long periods of amenorrhea followed by irregular bleeding
Polycystic Ovarian Syndrome • Life long history of irregular menses, hirsutism, infertility, and obesity is suggestive of PCO • Family Hx of PCO
Polycystic Ovarian Syndrome • Pelvic • ovarian enlargement-irregularity suggestive of cysts • clitoral hypertrophy • Breasts • Galactorrhea • Suggestive of hyperprolactinemia
(A) Pelvic ultrasound examination • Transvaginal ultrasound is the best imaging mode • Endometrial thickness should always be assessed to exclude significant endometrial pathology
Ultrasound assessment of the Polycystic ovaries International consensus definitions • Although the 1990 National Institute of Health Conference on PCOS recommended that diagnostic criteria should include evidence of hyperandrogenism and ovulatory dysfunction, in the absence of non-classic adrenal hyperplasia, and that evidence of polycystic ovarian morphology was not essential, the Rotterdam ESHRE/ASRM-sponsored PCOS consensus considered that PCO should be considered as one of the possible criteria for PCOS.
Ultrasound assessment of the Polycystic ovaries International consensus definitions • The PCO should have at least one of the following: either 12 or more follicles measuring 2-9 mm in diameter or increased ovarian volume (>10 cm3). If there is evidence of a dominant follicle (>10 mm) or a corpus luteum, the scan should be repeated during the next cycle. • The subjective appearance of PCOs should not be substituted for this definition. The follicle distribution should be omitted as well as the increase in stromal echogenicity and/or volume. Although the latter is specific to polycystic ovary, it has been shown that measurement of the ovarian volume is a good surrogate for the quantification of the stroma in clinical practice.
Ultrasound assessment of the Polycystic ovaries International consensus definitions (continued) • Only one ovary fitting this definition or a single occurrence of one of the above criteria is sufficient to define the PCO. The presence of an abnormal cyst or ovarian asymmetry, which may suggest a homogeneous cyst, necessitates further investigation. • This definition does not apply to women taking the oral contraceptive pill, as ovarian size is reduced, even though the `polycystic' appearance may persist.
Ultrasound assessment of the Polycystic ovaries International consensus definitions (continued) • A woman having PCO in the absence of an ovulation disorder or hyperandrogenism (`asymptomatic PCO') should not be considered as having PCOS, until more is known about this situation. • In addition to its role in the definition of PCO, ultrasound is helpful to predict fertility outcome in patients with PCOS (response to clomiphene citrate, risk for ovarian hyperstimulation syndrome (OHSS), decision for in-vitro maturation of oocytes). It is recognized that the appearance of PCOs may be seen in women undergoing ovarian stimulation for IVF in the absence of overt signs of PCOS. Ultrasound also provides the opportunity to screen for endometrial hyperplasia.
Ultrasound assessment of the Polycystic ovaries International consensus definitions (continued) • The following technical recommendations should be respected: • State-of-the-art equipment is required and should be operated by appropriately trained personnel. • The transvaginal approach should be preferred, particularly in obese patients. • Regularly menstruating women should be scanned in the early follicular phase (days 3±5). Oligo-/amenorrhoeic women should be scanned either at random or between days 3±5 after a progestogen-induced bleed. • If there is evidence of a dominant follicle (>10mm) or a corpus luteum, the scan should be repeated the next cycle. • Calculation of ovarian volume is performed using the simplified formula for a prolate ellipsoid (0.5 3 length 3 width 3 thickness). • Follicle number should be estimated both in longitudinal, transverse and antero-posterior cross-sections of the ovaries. Follicle size should be expressed as the mean of the diameters measured in the three sections.
The usefulness of 3-D ultrasound, Doppler or MRI for the definition of PCO has not been sufficiently ascertained to date, and should be confined to research studies.
Hormone assays • Blood tests needed to exclude ? • Late-onset congenital adrenal hyperplasia (17-hydroxyprogesterone) • Thyroid abnormality (TSH) • Hyperprolactinaemia (prolactin) • Cushing’s syndrome • These tests can be omitted if other features are not suggestive.
Androgens • testosterone (total or adjusted for SHBG) is helpful to showhyperandrogenaemia and to rule out an androgen-secreting tumour • Total testosterone concentration greater than 60 ng/dL ; consistent with PCOS • dehydroepiandrosterone sulfate and androstenedione is not particularly useful.
Insulin resistance • It is essential to exclude glucose intolerance with glucose tolerance testing • It is doubtful whether insulin measurement is indicated, as interpretation is clouded by obesity • calculating an index of insulin resistance from glucose and insulin levels (eg, the homeostasis model assessment [HOMA] or quantitative insulin sensitivity check index [QUICKI])
random and fasting glucose levels are usually normal in women with PCOS, the standard Australian recommendations for diagnosing diabetes by measuring these levels are not applicable, and glucose tolerance testing is recommended
Lipid status • Assessment of lipid status is justified - total and HDL cholesterol - triglyceride levels