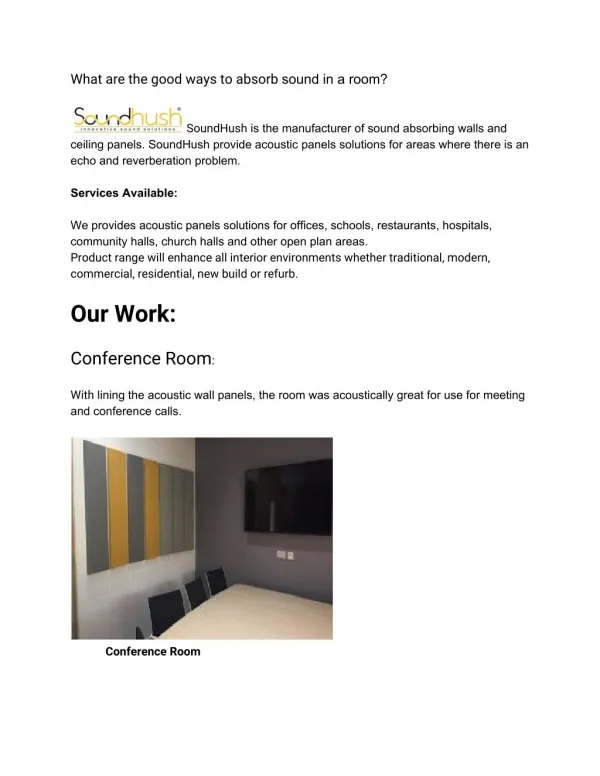
Physician Panels
Workers Compensation Program HomeTown Health HR Workshop March 16, 2010 presented by Ron Graves, Assistant Vice President Loss Control Anne Burleson, Director of Workers Compensation Sandy Carroll, Claim Supervisor Key Risk Insurance Company Key Risk Management Services, LLC.

Physician Panels
E N D
Presentation Transcript
Workers Compensation ProgramHomeTown Health HR WorkshopMarch 16, 2010presented byRon Graves, Assistant Vice President Loss Control Anne Burleson, Director of Workers Compensation Sandy Carroll, Claim SupervisorKey Risk Insurance CompanyKey Risk Management Services, LLC
Physician Panels • GA 34-9-201 • At least six physicians • One orthopedic surgery • No more than two industrial clinics • Employee selection • One change allowed 10.03.10.120
Employer Responsibility • Post the panel according to guidelines • Ensure employee understands function • Provide proper assistance 10.03.10.120
Plaintiff Attorney • Request copy of panel with notification of representation • Verify providers taking patients and still practicing • Name authorized treating physician if panel is found invalid. 10.03.10.120
Medical Authorizations • 34-9-207 • Refusal of an employee to sign release for medical information may effect his entitlement to compensation. 10.03.10.120
State Board of Workers Compensation Changes at the board: • Two new Board Directors:a) Chairman Rick Thompsonb) Judge Steven Farrow • Office closingsa) Gainesvilleb) Rome • No longer hearing cases in Forest Park • Administrative Law Judges – rotation 10.03.10.120
A Transitional Duty Program Is... • A managed care system designed to return injured employees back to their original job with minimal time lost • Designed to return injured workers to full capacity with minimum disability and maximum cost savings • Designed to help injured employees recover and return to medically approved work as soon as possible after an injury. This is a joint responsibility of: • The employer • The workers compensation claims adjuster • The medical case manager 10.03.10.120
To the employer Increased productivity Improved morale Reduced overtime Reduced temporary help Reduced claims costs To the employee Improved financial stability Faster recovery Eliminates separation Positive self esteem Continued work routine Benefits of a Transitional Duty Program 10.03.10.120
The Aging Workforce • U.S. work force is aging • Medium age in 2008 was 41 vs. 37 in 1990 • Workers delaying retirement *All stats are from U.S. Department of Labor 10.03.10.120
Older workers have more lost time from work Ages 35-44 8 days Ages 45-54 10 days Ages 55-64 11 days Ages 65 + 12 days • Workers 65 and over are working full time jobs at a higher rater. In 1995 it was 44%; in 2007 it was 57%. • The older the employee, the greater potential for more complications in the healing process from co-morbidities. 10.03.10.120
Medical Cost Drivers • Increase in severity • Patient care extending longer than normal period of time • Surgical recommendations increasing • Narcotic medications used earlier in treatment plan and ongoing • More medical disciplines involved in treatment, ex orthopedic, pain management, • More contentious litigation • Protection of Medicare's interest • Reduction of bringing employees back to work –economy 10.03.10.120
Medical Bill Adjudication • Our medical bill adjudication system utilizes a sophisticated rules based system in combination with the expertise of our trained medical bill review team. • CompCareLX™ is Key Risk’s layered network program. • Your clients’ utilization of the layered network drives network penetration resulting in additional savings when an injury occurs. • GA network penetration exceeds 93% (as of Jan 2010). 10.03.10.120
Medical Bill Review Process • Orthopedics & Sports Medicine – GA • Bill Details: • Dx1: 840.4 Sprain Rotator Cuff • Proc Code Description Charges • Repair Cuff $2,699.00 • 29826-59 Arthroscopy Shoulder 1,903.00 • 29825-59 Arthroscopy Shoulder 1,660.00 • 23412-80 Repair Cuff 674.75 • 29826-80 Arthroscopy Shoulder 475.75 • 29825-80 Arthroscopy Shoulder 415.00 • Total Charges $7,827.50 • Total Charges: $7,827.50 • Standard Fee Schedule Reductions - GA • - $758.65 • Additional Reductions from applying Key Risk Audit Rules • $3,353.89 • Additional Reductions from Key Risk's Nurse Review of Treatment and Bill Coding • $898.39 • Key Risk’s CompCare LX Savings • $1,334.72 • Total Savings: $6,345.65 • Paid Charges: $1,481.85 Each bill is systematically reviewed and fee schedule rules are interpreted and applied, the system marks bills needing additional review Each bill is adjudicated to State Fee Schedule or the usual and customary rate schedule Medical bills are analyzed by a Medical Savings Auditor, including Registered Nurses, for “Additional Savings” Each bill has Network Discounts applied where appropriate 10.03.10.120
Working Together. Delivering Better Outcomes. 10.03.10.120
Additional Resources: • Loss Control: Resources for our clients • Library of training videos • Links to helpful websites • Web Based Tools • Claims: Claims Management Tools • CompCare provider network • Web Tools – Network Pharmacy Locator, Employer/Employee • Procedures, Authorization for Release of Information Visit our website at www.keyrisk.com. State Board of Workers Compensation Website –www.sbwc.georgia.gov 10.03.10.120
SB 1788 “Nurse and Health Care Worker Protection Act of 2009” 10.03.10.120
Sponsorship and Referral Mr. Franken, Sponsor Committee on Health, Education, Labor, and Pensions 10.03.10.120
Purpose To reduce injuries to patients, direct-care registered nurses, and all other health care workers by establishing a safe patient handling and injury prevention standard. 10.03.10.120
Background • Direct care nurses rank 7th in the number of cases of musculoskeletal disorders resulting in days away from work • Nurses aides, orderlies, and attendants sustain the second highest frequency of musculoskeletal disorders of any occupation 10.03.10.120
Study Results 52% of nurses complain of chronic back pain and 38% suffer from pain severe enough to require leave from work. 10.03.10.120
Premise • Patients are not at optimum levels of safety while being lifted, transported, or repositioned manually. • Mechanical lift programs can substantially reduce skin tears suffered by patients and the frequency of patients being dropped. 10.03.10.120
Facts • A growing number of health care facilities have incorporated patient handling technology and have reported positive results. • As a result, the number of lost work days due to injury and staff turnover has declined. • Assistive patient handling technology successfully reduces workers compensation costs for musculoskeletal disorders. 10.03.10.120
Premise • Establishing a safe patient handling and injury prevention standard is a critical component in: • Protecting nurses and other health care workers • Addressing the nursing shortage • Increasing patient safety 10.03.10.120
Rulemaking • Within one year of the enactment of this Act, OSHA shall propose a standard on safe patient handling and injury prevention. • Within two years of the enactment of this Act, a final standard shall be promulgated. 10.03.10.120
Requirements • Engineering controls shall be used to perform lifting, transferring, and repositioning of patients. • Manual lifting of patients by direct care nurses and all other health care workers shall be eliminated. • The lone exception is where the safe use of patient handling practices can be demonstrated to compromise patient care. 10.03.10.120
Timing • Develop and implement a safe patient handling and injury prevention plan within six months of the promulgation of the standard that includes: • Hazard identification • Risk assessments • Control measures • Purchase, use, maintain and have accessible an adequate number of safe lift mechanical devices within two years of the promulgation of the standard. 10.03.10.120
Employee Participation Each employer shall obtain input from health care workers in developing and implementing the safe patient handling and injury prevention plan, including the purchase of equipment. 10.03.10.120
Data Collection Establish and maintain a data collection system that tracks and analyzes trends in injuries and make such data and analyses available to employees. 10.03.10.120
Documentation of Exceptions Document each instance when safe patient handling equipment was not used due to legitimate concerns about patient care and generate a written report in each instance that includes: • The work task being performed • The reason the equipment was not used • The nature of the risk posed to the worker • The steps being taken to prevent a similar situation 10.03.10.120
Training Frequency Train nurses and other health care workers on safe patient handling and injury prevention policies, equipment, and devices at least annually. 10.03.10.120
Training • Include information on hazard identification, assessment, and control of musculoskeletal hazards. • Conducted by an individual with knowledge in the subject matter • Delivered, at least in part, in an interactive classroom-based and hands-on format. 10.03.10.120
Posting Requirements Post a notice that: • Explains the standard • Includes information on policies and training • Explains procedures to report patient handling-related injuries 10.03.10.120
Annual Evaluation Conduct an annual written evaluation that includes: • Handling procedures • Selection of equipment • Engineering controls • Assessment of injuries • New safe patient handling and injury prevention technology 10.03.10.120
Evaluation Team The annual evaluations shall be conducted with the involvement of nurses, other health care workers and their representatives and be documented in writing. 10.03.10.120
Follow-up Heath care employers shall take corrective action as recommended in the written evaluation 10.03.10.120
Refusal of Assignment A health care worker may refuse to accept an assignment from a health care employer if: • The assignment would subject the worker to conditions that would violate the standard. • The worker has not received the required training. 10.03.10.120
Worker Protection • No employer shall discharge, discriminate, or retaliate in any manner against a worker based on the worker’s refusal of a lifting assignment. • No employer shall file a complaint or a report against a worker with a state disciplinary agency because of a refusal of a lifting assignment. • No employer shall discriminate or retaliate against a worker who, in conjunction with another worker: • Reports a violation or suspected violation of the standard • Investigates, cooperates, or participates in an investigation • Informs or discusses with individuals a violation or suspected violation 10.03.10.120
Notice Health care employers shall include a notice explaining the rights of workers and including a statement that a worker may file a complaint with the Secretary (OSHA) against an employer that violates the standard, including instructions for how to file a complaint. 10.03.10.120
Grants The Secretary of Health and Human Services shall establish a grant program that provides financial assistance to cover some or all of the costs of purchasing safe patient handling and injury prevention equipment for health care facilities. 10.03.10.120
Grant Requirements Hospitals, nursing facilities, home health care, and outpatient facilities must show that • Such equipment is required to comply with the standard and • Demonstrate the financial need for assistance with purchasing the equipment. 10.03.10.120
Authorization of Appropriations There are authorized to be appropriated for financial assistance $200,000,000 of which $50,000,000 will be available specifically for home health agencies or entities. 10.03.10.120
Thank you for joining us today! 10.03.10.120