Download
1 / 33
330 likes | 400 Views
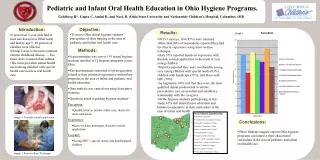
Explore the benefits of one-year oral evaluations in pediatric dentistry, endorsed by AAPD, ADA, and more. Overcome common objections and learn to integrate preventive care for infants. Adopting early dental exams can enhance practice profitability, build rapport with parents, and prevent dental issues in children. Find out why it's essential to start infant oral health programs and reach out to internal, professional, and public communities for successful implementation. Educate staff, engage in risk assessment, and streamline appointment scheduling for effective incorporation. Stay updated with common FAQs, risk assessment tools, and clinical staff orientation to provide quality infant oral care, emphasizing preventive strategies.

E N D
INFANT ORAL HEALTH Making it work in your office Ray E. Stewart DMD, MS
“ The greatest obstacle to getting and infant program up and running in my office was to convince my staff and employees that it all made sense.” -Anonymous Pediatric Dentist
There is a growing acceptance of the validity and efficacy of the one year examination. The following organizations and agencies have endorsed and adopted policies that support it. AAPD ADA AAGD AAP AAPHD
The purpose of this session is to provide the pediatric dentist with the motivation to consider an infant program in his/her practice if they haven’t done so already, and for those who have, to provide some thoughts and ideas as to how to make it a profitable and enjoyable experience.
For those who have yet to embrace the concept of the one year oral evaluation I would point out that it has been AAPD policy since 1995? THE TRAIN HAS LEFT THE STATION!!!
We hear many reasons why practitioners do not perform the age one infant oral evaluation. • Existing conditions should dictate when a patient is seen, not his/her age. • Parents don’t see the reason for or value of the infant oral exam. • There is very little decay in the community where I practice. • Parents should decide when their child should be seen by the dentist. • Patients are not cooperative at this age. • I am to busy treating older patients and seeing infants would be disruptive to my office routine. • It is difficult to get insurance to reimburse for infant exams. • Infant oral exams frighten the child. I don’t want to create a “dental phobic”.
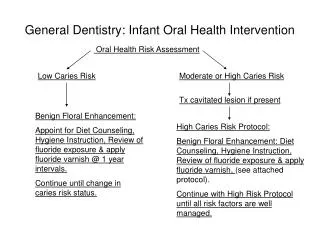
REASONS FOR EMBRACING THE 1 YEAR DENTAL EXAMIt is easy to do It is a great diversion to the pediatric dental office routine.It can be profitable.It can be a great practice builder.It is greatly appreciated as an educational opportunity by parents.It provides an early opportunity to truly prevent dental disease. PREVENTIVE vs REACTIVE
THE MOST COMPELLING REASON TO ADOPT THE 1 YEAR DENTAL EXAM IS “If we don’t do it someone else will”
“Into the Mouths of Babes” a program initiated in North Carolina in1999 was expanded state wide in 2001 enabling private practice physicians, physicians and RN’s to apply fluoride varnish in Medicaid children ages birth to three and be reimbursed for the services
California now reimburses physicians for applying fluoride varnish as a means of preventing EEC. • Seven states now permit the unsupervised practice of dental hygienists. • Forty-four states now allow “general supervision” of dental hygienists.
WHERE TO BEGIN? • Once the decision is made to incorporate an IOH program into your practice there are three primary areas on which to focus to assure success
THREE COMMUNITIES WE NEED TO REACH • INTERNAL Staff and Employees Patients (families) of record • PROFESSIONAL Dentists Physicians, Nurses, PA’s 3. PUBLIC
FIRST AND FORMOST We need buy-in and total acceptance of the concept from our staff and employees. To get this buy-in they need to be educated! Infectious disease paradigm Dental Home Concept Caries Risk Assessment Anticipatory Guidance Motivational Interviewing
RECEPTION/FRONT OFFICE STAFF 1. In-service power point presentation (30-40 minutes) covering rationale of IOH exam. 2. How to answer FAQ’s 3. Introduction to Caries Risk Assessment 4. Motivational Interviewing
FREQUENTLY ASKED QUESTIONS: “My pediatrician suggested that I make a dental appointment for my 11 month old daughter. She only has six teeth, why on earth does she need to see a dentist?”
My pediatrician told me to take my son to the dentist when his first tooth comes in but my dentist says he does not want to see him until he is three or four. What should I do?
“My 18 month old baby does not like strangers! I know she will just pitch a fit if I bring her in for an appointment. What will you be doing on the first visit?
Initial contact is a good time to introduce the concept of Caries Risk Assessment. All team members should be familiar with the tool that you use, how it is administered, and how it is used to identify infants who are at increased risk for developing ECC.
RISK ASSESSMENT TOOLS AAPD CAMBRA California DHCS
RISK GROUPS COMMON TO ALL CAT’S • Children with special health care needs • Children of mothers with high caries rate • Children demonstrating significant plaque, staining, demineralization, or caries. • Children who sleep with a bottle or breastfeed throughout the night. • Later-order offspring • Children from families of low socioeconomic status.
SCHEDULING BLOCK OR INTEGRATED? Depending on office policies or scheduling preferences IOH exams can be integrated into the regular office schedule as any new patient exam or block scheduled as IOH exams only on a particular day and time of day.
CLINICAL STAFF ORIENTATION 1. Modify power point for clinical emphasis. 2. Knee to knee exam 3. Armamentarium and tray set up 4. Perform risk assessment 5. Anticipatory guidance
KNEE TO KNEE (CLINICAL) EXAM What to look for: Plaque and inflammation Stains Demineralization (white spot lesions) Decay
KNEE TO KNEE EXAM What to do: Lift the lip demonstration Toothbrush prophy and Home Care instruction Silver Diamine Fluoride application Fluoride varnish application (where indicated)
THREE SEPARATE BUT INTEGRALLY RELATED APPROACHES TO SUCCESSFULLY IMPLEMENTING AN IOH PROGRAM
POINTS OF LIGHT A turnkey program by Dr Kevin Hale for establishing an Infant Oral Health program in your community. This program is based on the collaborative interaction of dentists and pediatric medical providers to achieve the goal of having all infants receive an Oral Health Risk Assessment and establishment of a Dental Home by age one.
1. ENHANCEMENT OF CHILDRENS ORAL HEALTH BY EDUCATING MEDICAL CARE PROVIDERS
Emphasize importance of one year Infant Oral Health evaluation to Pediatricians and other Primary Care Providers in your community. Provide instruction and guidance on: a) Caries Risk Assessment b) Oral Health Evaluation c) Appropriate referral to Dental Home d) Application of fluoride varnish in moderate and high risk infants when referral not possible.
ENHANCEMENT OF CHILDRENS ORAL HEALTH BY EDUCATING DENTISTS IN YOUR COMMUNITY ON HOW TO COMPLY WITH ADA/AAPD GUIDELINES ON ESTABLISHMENT OF DENTAL HOME BY AGE ONE.
ESTABLISHMENT OF A DENTAL HOME • With 5 million plus Dentical children in California alone, it should be quite evident that the 600 practicing Pediatric Dentists throughout the State can not begin to provide Dental Homes for all of the at risk children in the population. • WE NEED GENERAL DENTISTS TO ADOPT INFANT ORAL HEALTH AS A PRIORITY!!!