Download
1 / 1
10 likes | 123 Views
Innovative Use of Social Media Tools to Enhance Retention in Community-based Research. Gloria M. Miele, Ph.D. 1 , Aimee N. C. Campbell, Ph.D. 1,2 , Eva Turrigiano 2 , Edward V. Nunes, M.D. 1, 2 Columbia University College of Physicians and Surgeons, (2) New York State Psychiatric Institute.

E N D
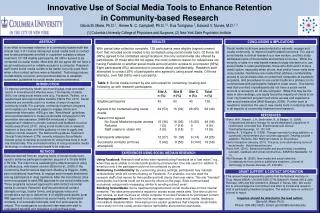
Innovative Use of Social Media Tools to Enhance Retention in Community-based Research • Gloria M. Miele, Ph.D.1, Aimee N. C. Campbell, Ph.D.1,2, Eva Turrigiano 2, Edward V. Nunes, M.D.1, 2 • Columbia University College of Physicians and Surgeons, (2) New York State Psychiatric Institute ABSTRACT RESULTS CONCLUSIONS & IMPLICATIONS In an effort to increase retention in a community-based multi-site clinical trial, 3 of 10 sites introduced social media tools to contact and locate participants enrolled in outpatient substance abuse treatment. Of 138 eligible participants, 68 (49%) agreed to be contacted via social media. Most who did not agree did not have a social media account or reliable access to a computer. Research staff found social media outlets to be useful, but only used them when other contact options were exhausted. Technology issues, confidentiality concerns, and recommendations to establish systematic guidelines for social media use are presented. With partial data collection complete, 138 participants were eligible (signed consent form that included social media) to be contacted using social media tools. Of those, 68 (49%) agreed to be contacted using Facebook, the only social media site offered by participants. Of those who did not agree, the most common reason for refusal was not having Facebook or another social media account and/or access to a computer (36%). Eight participants (6%) refused due to concerns about confidentiality. Research staff attempted to contact 25% of participants who agreed to using social media. Of those attempts, over half (56%) were successful. Social media tools have great potential to educate, engage and create community to improve health-related outcomes. The use of social media in clinical research is a new venture, and this study addresses some of the benefits and barriers to its use. While the minority of sites in a web-based research study elected not to use social media to retain participants, those who did found it to be a useful option, especially when phone, mail and/or home visits were unsuccessful. Guidelines are needed that address confidentiality, access to social media sites on networked computers at treatment programs, and procedures to use social media as a primary tool to communicate with participants instead of a last resort. One barrier was that one-third of participants did not have a social media account or access to an off-site computer. While this may be the case in other settings, one study found the majority of clients at an inner city treatment program had online access and experience with social media sites (Wolf-Branigin, 2009). Further work is needed to maximize the use of new media tools in retaining clients in all aspects of community treatment and research. INTRODUCTION To improve community health, we must engage, treat and retain clients in innovative and effective ways. The majority of adults (65%) are using social media tools (e.g., Facebook, Twitter), on a regular basis and report positive benefits (Harris Poll, 2011). Social networks are currently used in a number of ways to improve community health. For example, community treatment programs and hospitals use Facebook pages to engage clients and disseminate information. AIDS.gov has “New Media” guidelines and recommendations to create social media campaigns for HIV prevention and education. SAMHSA introduced a “digital engagement” initiative to provide outreach and feedback to social media users (Pond, 2011). Using social media tools in research, however, is less clear, with little guidance on how to apply new media to clinical research. The National Drug Abuse Treatment Clinical Trials Network (CTN) recently initiated a Social Media interest group to develop procedures for using these tools in multi-site clinical trials. This uncharted territory of using innovative media technology in clinical research needs to be explored. REFERENCES Bickel, W.K., Marsch, L.A., Buchhalter, A., & Badger, G. (2008). Computerized behavior therapy for opioid dependent outpatients: A randomized, controlled trial. Experimental and Clinical Psychopharmacology, 16, 132-143. Budney, A., & Higgins, S. (1998). Therapy manuals for drug addiction, a community reinforcement plus vouchers approach: Treating cocaine addiction.Rockville, MD: National Institute on Drug Abuse. Harris Interactive (January, 2011). The pros, cons and learning curve of social media. Harrisinteractive.com. Pond, M.H. (2011). Behavioral health and social media: Increasing outreach, feedback and virtual communities. SAMHSA Newsletter, 19 (1). Wolf-Branigin, M. (2009). New media and social networks: Considerations from clients in addictions treatment. Journal of Technology in Human Services, 27, 339-345. METHODS EXPERIENCES USING SOCIAL MEDIA IN RESEARCH Data are derived from an ongoing study of social media tools used to enhance participant retention as part of a 10-site NIDA CTN trial. The main trial is evaluating the effectiveness of using an efficacious, web-based version (Bickel et al., 2008) of the Community Reinforcement Approach (Budney & Higgins, 1998), plus motivational incentives, to engage and increase abstinence among participants in drug treatment. After the trial started, sites were encouraged to seek IRB approval to use social media tools. Three programs received approval to add contact via social media to consent. Research staff documented all contact attempts on logs, locator forms, and progress notes and completed a survey to determine: # of eligible participants (post IRB-approval) to be contacted via social media; # attempted contacts; # of successful attempts; and # of and reasons for refusal. The investigators conducted interviews with staff to understand benefits and obstacles to using these tools. Using Facebook: Research staff at two sites reported using Facebook as a “last resort,” e.g., when they were unable to contact participants by phone/email. One site used it in addition to email but only if the participant could not be contacted by phone. Maintaining Confidentiality: By customizing privacy settings, participants may maintain confidentiality while still communicating on Facebook. For example, one site used the research staff’s first names for their profile and told clients their user name. This site “friended” participants, but friends could not be seen by others on the page. Sites communicated exclusively using private messaging, similar to sending a direct email. Blocking Social Media: Some treatment programs block social media sites on their internal networks. Two sites were granted a request to access social media sites. One site could not gain access, so staff must use an offsite computer to access Facebook for participant contact. Developing guidelines: Each site had its own approach to using social media, leading to inconsistent implementation. Developing more explicit guidelines that integrate social media into a study from the outset would improve replicability and potential usefulness. GRANT SUPPORT & CONTACT INFORMATION This research was supported by grants from the National Institute on Drug Abuse (NIDA): U10 DA13035 (CTN; Edward V. Nunes, MD & John Rotrosen, MD) and K24 DA022412 (Edward V. Nunes, MD). We would like to acknowledge the commitment and effort of clinical and research staff at participating treatment programs. The authors have no conflict of interest to report. Inquiries should be directed to the lead author: Gloria M. Miele, Ph.D. Phone: 805-482-1625 | Email: gmm23@columbia.edu