High Alert Medication
High Alert Medication. Definition:. medication that have a higher likelihood of causing injury if they are misused. Errors with these medications are not necessarily more frequent- just their consequences may be more devastating. Some high alert medications also have high volume use.

High Alert Medication
E N D
Presentation Transcript
Definition: • medication that have a higher likelihood of causing injury if they are misused. Errors with these medications are not necessarily more frequent- just their consequences may be more devastating. Some high alert medications also have high volume use.
TOP FIVE HIGH ALERT MEDICATIONS • Insulin • Opiates and narcotics • Injectable potassium chloride or phosphate concentrate • Intravenous anticoagulants (heparin) • Sodium chloride solutions above 0.9 percent. Ref. ISMP 2007 Survey on High-Alert Medications
INSULINCommon risk factor: • Lack of dose check systems • Insulin & heparin vials kept in close proximity to each other on a nursing units, leading to mix-ups • Use of “U” or “IU” • Incorrect rates being programmed into an infusion pump
Suggested Strategies: • Establish a check system whereby one nurse prepares the dose and another nurse reviews it. • Do not store insulin and heparin near each other. • Spell out the word “units” instead of “U” • Build in an independent check system for infusion pump rates and concentration settings.
OPIATES AND NARCOTICSCommon risk factors: • Narcotics kept as floor stock • Confusion between morphine and hydropmorphone • PCA ( patient controlled analgesia) errors regarding rate and concentrations.
Suggested Strategies: • Limit opiates and narcotics in Floor stock • Education (sound-alike, hydromorph.) • Implement PCA protocols • Double-check drug and pump settings • Prepare infusion in Pharmacy
INJECTABLE POTASSIUM CHLORIDE OR PHOSPHATE CONCENTRATE Common risk factor: • Mixing pot. chloride/ phosphate • Request for unusual concentrations • Unclear labels • Storing concentrated potassium chloride/phosphate outside the pharmacy
Suggested strategies • Remove Pot. Chloride/ phosphate from wards • Use commercially available premixes • Standardize and limit concentrations • Prepare, double-check in pharmacy
INTRAVENOUS ANTICOAGULANTS (HEPARIN) Common risk factor: • Unclear labelling regarding concentration and total volume • Multidose-containers • Confusion between heparin and insulin due to similar measurement units and proximity.
Suggested strategies: • Standardized concentrations and use premixed solutions. • Use only single-dose containers. • Separate heparin and insulin.
SODIUM CHLORIDE SOLUTIONS ABOVE 0.9 PERCENT Common risk factor: • Storing sodium chloride solutions above 0.9 percent on nursing units. • Large number of concentrations/formulations available. • No double check system in place.
Suggested strategies: • Limit access of sodium chloride solutions above 0.9 percent and remove from nursing units. • Standardize and limit drug concentrations. • Double check pump rate, drug, concentration and line attachments.
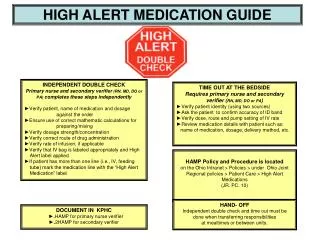
ACTIONS THAT CAN BE TAKEN IN CLINICAL AREAS • Risk awareness- be aware of high alert products in your area. • Review floor stock to reduce availability of items, as well as, quantities. • Use of shelf labelling which incorporates TALLman lettering. • Separate storage for easily mistaken medicines. • Additional product labels. • Read the labels three times (RL3). • Insure proper and correct programming of infusion pumps.
Independent double checking system ( example: IV medication and infusion pumps). • Standardize the prescribing / order entry/IV infusion labelling/pump settings. • Know the medications that you administer example dose, route, frequency, effect, common adverse effects, and monitoring ( laboratory
1. ELIMINATE THE POSSIBILITY OF ERROR • Reducing the number of medications in the formulary. • Reducing the number of concentrations and volumes to those clinically appropriate for most. • Remove / minimize high alert medications from clinical areas, where possible.
2. MAKE ERRORS VISIBLE • Have two individuals independently check the product or setting. Examples: IV pumps and epidural medications, insulin doses drawn up in syringe, and chemotherapy and TPN production.
3. MINIMIZE THE CONSEQUENCES OF ERROR. • Minimize the size of vials or ampules in the patient care area to the dose comonly needed ( example: heparin in single dose vial versus 10 ml vials • Reduce the total dose of High Alert Medications in continous IV drip bags(example: 12,500 units of heparin in 250 ml vs 25,000 units in 500 ml) to reduce risk when it runs away, because it will.