Hepatic / GI
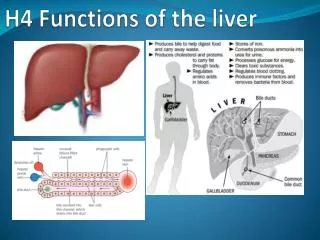
Hepatic / GI. At the end of this self study the participant will: Verbalize causes of hepatic failure and pancreatitis Describe assessment findings of the patient with liver disease and pancreatitis. Manufacture of heparin Modification of fats Manufacture of bile Manufacture of coags.

Hepatic / GI
E N D
Presentation Transcript
Hepatic / GI At the end of this self study the participant will: • Verbalize causes of hepatic failure and pancreatitis • Describe assessment findings of the patient with liver disease and pancreatitis.
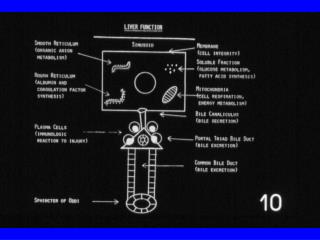
Manufacture of heparin Modification of fats Manufacture of bile Manufacture of coags Synthesis of ammonia to urea Plasma protein formation Drug/alcohol/hormone detox Synthesis of glycogen Hepatic Function
Amiodarone Phenytoin INH/Rifampin Sulfas Erythromycin Tricyclic Antidepressants Estrogen Acetaminophen Hydralazine Tetracycline Rezulin Lovastatin Common Medications that can be Hepatotoxic
Acetaminophen Toxicity • 8 gm (15 extra strength Tylenol) taken in a 24 hour period can cause significant liver damage. • It is recommended the general public do not exceed 4 gm/24 hours. • Consumption of > 4 alcoholic drinks/ day then recommendation decreased to not to exceed 2 gm/24 hours. • > 3 drinks/day = 4 oz. liquor, 4 beers, or 16 oz. wine.
Lab Tests • ALT – Elevated in alcohol abuse, gallstones, mononucleosis, medications, more specific for liver problems than AST • AST– Elevates in MI, bruised kidney, pancreas problems, and liver disease (with use/abuse of Alcohol, Statins & Tylenol) • Alk Phos– Elevated for extra- and intrahepatic biliary obstruction, sepsis. If elevated but GGPT normal, more likely bone disorder • GGPT-Most indicative of biliary obstruction (with alk phos).
Lab Tests • Bilirubin - Result of hemoglobin breakdown. • Elevates in liver failure R/T inability of liver to convert bili to soluble form. • Jaundice, itching, dark urine when total bili reaches 3 mg/dl • Serum Proteins – Albumin, Globulin & fibrinogen • Decreased with liver dz, starvation, malabsorption, poor iron intake • Increased with hemoconcentration: N/V/D, poor kidney function.
Coagulation • Prothrombin Time • PT normal 11.0-15.0 seconds • INR normal 0.81-1.20 • Physician alert value (automatic call back): >5.0 INR • Partial Thromboplastin Time • Ptt normal 23.0-36.0 seconds • Physician alert value (automatic call-back): >150 seconds
Ammonia • Protein metabolism: ammonia is converted to urea • Elevated levels affect acid-base balance, brain function (encephalopathy) • Asterixis (Liver flap) • Assessed by asking patient to hold arms out in front, hands dorsiflexed. Liver flap is a hand tremor in this position • To lower ammonia level • Lactulose, neomycin, low protein diet
Ascites Contributing factors low alb increased lymph portal htn Complications: bacterial peritonitis umbilical hernia hydrothorax Edema / anasarca Skin changes Bruising Jaundice Pruritis Assessment Ascites
Coagulopathy of liver disease • Decreased production of clotting factors • Increased consumption of clotting factors • Production of abnormal clotting factors • Increased bleeding • Internal • External • With interventions (e.g., IV insertion) • Spontaneous without provocation
Causes of Liver Dysfunction • Inflammatory Disorders- hepatitis • Toxins- environmental: huffing, inhaling pesticides, toxic work environments. • Drugs- Prescription and illicit. • Vascular Disorders- heart disease • Metabolic Disorders [Fatty Liver disease/NASH (Nonalcoholic Steatohepatitis)] • Neoplasms- cancers • *Most common cause of liver failure is drugs/alcohol and hepatitis C
Cirrhosis • Primary: Autoimmune • Secondary: Obstruction (such as stones) • Laennec’s: Alcoholic (50% of all causes) • Cardiac: Right heart failure • Postnecrotic: • After injury or circulatory obstruction • Infectious causes • Cryptogenic • No cause found – just happens
Body Fluid Transmission B, C, D, G Fecal-oral Transmission A, C(rare), E Contaminated Food Ingestion A Perinatal Transmission A, B, C, D Inflammation of the liver Only A and B have a vaccine C can be treated, however is the main cause of liver transplants D is parasitic to B. Cannot have hep D without B. E extremely rare in US, more prevalent in underdeveloped countries G has few symptoms in humans. Hepatitis
Esophageal Varices • Primarily caused by portal hypertension • High pressure causes backup of blood to organs normally drained by portal system • Dilated, engorged veins • Often bleed within one year after discovered(70% reoccurrence). • Bleeding painless and massive: difficult to control (60% stop spontaneously). • 90% of patients with cirrhosis have varices
Medical Management of Esophageal Varices • Sclerosing Therapy • Endoscopic procedure, medication (sterile water or epinephrine) injected into each varix • Scar tissue develops, closing off varix • Variceal Band Ligation • Endoscopic procedure, rubber band placed around varix • Varix becomes necrotic, falls off Variceal Band Ligation
Upper GI Bleed Causes • Main cause is ulcers and gastritis(4.5million Americans have ulcers). • Hypoxia of GI mucosa can disrupt mucosal barrier • Bacteria- h.pylori present in 95% of duodenal and 80% gastric ulcers – h.pylori can be protective, especially on esophagus • Cancer • Peptic Ulcers • Mallory Weiss Tear (protracted vomiting) • Esophageal Varices
Drug Therapy Proton pump inhibitors (e.g., Prilosec) H2 Blockers (ranitidine, famotidine). Antacids Sucralfate Reglan Upper GI Gastric Oversew Vagotomy Gastric Resection Gastrectomy Lower GI Resection Treatments Medical Surgical
Pancreatitis • Inflammatory process • Enzymes activated and released within the pancreas • Acute and chronic forms; edematous and hemorrhagic forms. • Severity ranges from edema to necrosis • A common mnemonic for the causes of pancreatitis spells "I get smashed", an allusion to heavy drinking (one of the many causes):
I - idiopathic G - gallstone. E - ethanol (alcohol) T - trauma (gunshot wounds, crush injuries)S - steroids M - mumps, other viruses (Epstein-Barr, Cytomegalovirus) A - autoimmune disease S - scorpion sting and also snake bites H - hypercalcemia, hyperlipidemia/hypertriglyceridemia and hypothermia E - ERCP (Endoscopic Retrograde Cholangio- Pancreatography) D - drugs (e.g., thiazides, NSAIDS, steroids and duodenal ulcers
Panreatitis Assessment • Abdominal pain • Greatest in the upper abdomen, may radiate to back • May last from hours to day, or continuous • May be worsened by eating, drinking and/or alcohol consumption • Nausea • Vomiting • Weight loss (On average patients with pancreatitis lose 6-12 pounds)
Pancreatitis Tests • Elevated: • Amylase (most common) • Lipase (most accurate) • Triglycerides • WBCs • Decreased: magnesium, potassium, calcium, albumin. • ERCP (yes, the same test that can cause pancreatitis is also done as a diagnostic measure)
Pancreatitis Treatment • Pain control !!! • NPO (N/G not required unless significant abdominal distention occurs) • Antibiotics may be considered for necrotizing or infectious forms • Surgery. Last resort (remember islets of langerhans) • Fluid replacement • Stop drinking alcohol and smoking (even if cause not alcohol consumption)