Download

1 / 67
740 likes | 939 Views
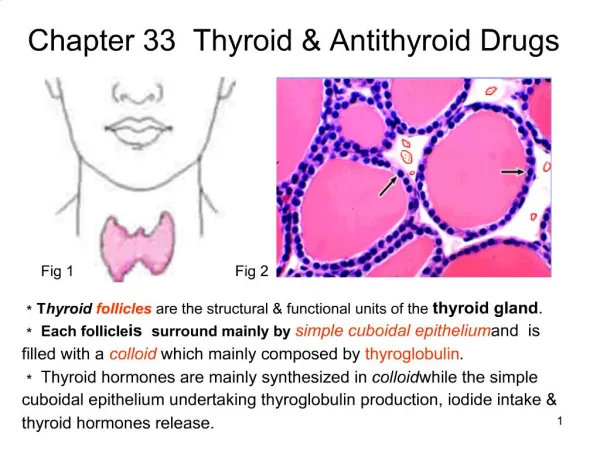
THYROID AND ANTI THYROID DRUGS. By : Dr. Abdul Latif Mahesar Department of medical pharmacology KKUH , King Saud University. Normal thyroid gland secretes T3 (triiodothyronine) and T4 (tetraiodothyronine). To maintain Normal growth and development of Nervous Skeletal

E N D
THYROID AND ANTI THYROID DRUGS By : Dr. Abdul Latif Mahesar Department of medical pharmacology KKUH , King Saud University
Normal thyroid gland secretes T3 (triiodothyronine) and T4 (tetraiodothyronine). To maintain Normal growth and development of • Nervous • Skeletal • Reproductive systems
It also controls metabolism of • Fats • Carbohydrates • Proteins and • Vitamins
and hence controls • Normal body temperature • Normal energy levels Thyroid status also affects Secretion and degradation of • Catecholamine • Cortisones • Estrogens • progesterone and • insulin
Mental retardation (Cretinism) and dwarfism results due to deficiency of thyroxine in early life. • Hyperactivity of thyroid resembles sympathetic over activity, this may be due to oversensitivity of β-adrenergic receptors or increase in their number. • There may also be increase in the production of catecholamines
increased epinephrine activity causes • Tremors • Sweating • Anxiety • Nervousness • lid lag retraction
Manifestations of Hyperthyroidism • Restlessness , nervousness , irritability. • Tremors • palpitation • Weight loss • sweating • Heat intolerance
|Manifestations cont’d • Diarrhoea • Short breath • Itching • Tiredness • Light periods • Exophthalmos
Manifestations of Hypothyroidism • Fatigue and lack of energy • weight gain • Dry and cold skin • Dry hairs • Constipation • Slowed thinking • Bradycardia • Heavy menses • Intolerance to cold
Causes of hypothyroidism • Drugs • Auto immune destruction • Blocked hormone formation • Impaired synthesis of T4 • Destruction or removal of gland • Iodine deficiency • Receptor blocking antibodies • pituitary or hypothalamic disease.
SYNTHESIS OF THYROID HORMONES • Iodide , an ions is actively taken up by the thyroid gland (Iodine trapping)/iodine uptake • Iodine is stored in the thyroid and is concentrated 25 times more • Iodide an ion is then oxidized to iodine by thyroidal peroxidase.
It iodinates tyrosine (with in thyroglobulin, a glycoprotein molecule) to form mono-iodotyrosine (MIT) and Di-iodotyrosine (DIT), called organification or iodination.
Biosynthesis of thyroid hormones ,also showing various sites of anithyroid drug actions
Two molecules of DIT unite to form T4 (tetra- iodothyroine) and one molecule of MIT and DIT combine to form T3 (tri-iodothyronine). • These hormones are released by exocytosis and proteolysis of thyroglobulin. • Ratio of T4 to T3 in thyroglobulin is 5:1 • Most of T3 in circulation is derived from metabolism ofT4.
HORMONE TRANSPORT. • T4 and T3 are reversibly bound to thyroxine binding globulin (TBG). • 0.04% of total T4 and 0.4% of T3 exist in free form • Starvation , pregnancy , steroid hormones affects their binding
Metabolism of thyroxine in to active T3 and inactive T3 (rT3)
PERIPHERAL METABOLISM • Small amount is biologically inactivated by deamination, decarboxylation conjugation and excreted as Glucuronide or sulphate, but • The primary pathway of peripheral thyroxine metabolism is DEIODINATION. • Deiodination of T4 at outer ring to active and 3-4 times more potent T3. and
Metabolism cont’d • De-Iodination of inner ring produces reverse T3(rT3), metabolically inactive. • Drugs like ipodate, β-blockers and corticosteroids; starvation inhibits 5-deiodinase. • This results low T3 and high rT3.
Hypothalamic –pitutary – thyroid axix Thyroid regulation
THYROID REGULATION • Thyrotropin releasing hormone (TRH) is secreted by hypothalamic cells in pituitary portal venous system. • It acts on pituitary and causes synthesis and release of thyroid stimulating hormone (TSH). • This in turn acts on thyroid cell to increase release and synthesis of T3 and T4.
These thyroid hormones in a negative feed back fashion act on pituitary to block action of TSH and on hypothalamus to inhibit TRH. • Level of iodine in blood also regulates thyroidal secretion independent of TSH. (large doses of iodide inhibits iodine organification) • THYROXINE ISOMERS: Naturally occurring molecules are L- isomers; where as synthetic molecules are D-isomers. D -isomers have only 4% activity of L-isomers.
T3 T4 T3 PP T3 T3 T4 T3 T3 PB Pre-m RNA cytoplasm Nucleus Response mRNA Protein Mechanims of action of thyroid hormones Mechanism of action of thyroxine at cellular level
MECHANISM OF ACTION • Free form of T3 and T4 enter cell by diffusion /active transport . T4 is converted to T3 and enters nucleus and binds to T3 receptors, this leads to increased formation of mRNA and subsequent protein synthesis.
Pharmacokinetics of administered thyroid hormones • T4, best absorbed in duodenum and ileum, this can be altered by food and drugs, such as calcium preparations and antacids containing aluminum, intestinal flora Absorption of T4 is 80% and of T3 is 95%. • Absorption is not affected by mild hypothyroidism but impaired in myxedema with ileus, for this parental route is preferred.
In hyperthyroidism metabolic clearance of T3 and T4 is increased and their half life is decreased and opposite is true in hypothyrodism. • Enzyme inducers increase metabolism of T3 and T4 but concentration is maintained in euthyroid. • Same compensatory mechanism occurs if binding sites are altered as in pregnancy, estrogen therapy and use of oral contraceptives.
Thyroid preparations • LEVOTHYROXINE:(T4) • This is the preparation of choice for thyroid replacement and suppression therapy, because it is stable and has a long (7 days) half life, to be administered once daily. • Oral preparations available are from 0.025 to 0.3 mg tablets • For parentral use 200-500µg (100µg/ml when reconstituted) for injection.
LIOTHYRONINE(T3) : • This is more potent (3-4 times) and rapid acting than levothyroxine but has a short half life (24 hours) compared to levo, is not recommended for routine replacement therapy, it requires multiple dosing in a day. • It should be avoided in cardiac patients. • Oral preparation available are 5-50µg tablets • For parentral use 10µg/ml
Comparison of T4 to T3 • T4 production is more than T3 • T4 is converted to T3 in periphery • T3 is more potent than T4 • T3 acts faster thanT4 • T3 enters cell easily than T4 • T3 binds to receptors in nucleus.
ANTITHYROID AGENTS: • Mechanism • Agents which interfere production of thyroid hormone . • Agents which modify tissue response to thyroid hormones • Glandular destruction with radiation or surgery.
Drugs : • Thioamides • Iodides • Radio active iodine • Iodinated contrast media • Adrenoceptor- blocking Agents • Anion inhibitors
THIOAMIDES: • Methimazole • Carbimazole • Propylthiouracil • Methimazole is 10 times more active than propylthiouracil.
Mechanism of Action • They act by: • Inhibiting thyroidperoxidase –catalysed reaction to block iodine organification. • They block coupling of iodotyrosine • They inhibit peripheral Deiodination of T4 to T3. • Onset of drug is slow requiring 3-4 weeks before stores of T4 are depleted.
Pharmacokinetic comparision between Propylthiouracil and Methimazole
Pharmacokinetic comparision between Propylthiouracil and Methimazole
Adverse Effects ( thioamides) • It occurs in 3-12 % of treated patients • Maculopapular rash and fever are earlier effects. • Urticarial rash, vasculitis, arthralgia ,cholestetic jaundice ,lymphadenopathy, and hypoprothrombenemia. • Most dangerous complication is agranulocytosis this is infrequent but may be fatal.
IODIDES: • They inhibit organification and hormone release. With a dose of > 6 mg /day. • They should be initiated after onset of thioamides therapy. • It also decreases the vascularity of hyperplastic gland (making it valuable for preparation for surgery) • Improvement israpidwithin2-7 days (valuable in thyroid storm) • Should not be used alone ! ?
Iodides cont’d • Well and rapidly absorbed from intestines • Rapidly taken by thyroid gland and concentrated there • Moderate increase leads to hormone secretion but substantial excess inhibits hormone release and promotes its storage, making the organ less vascular and firmer. • iodides stores in thyroid delays response to thioamides
Precautions /toxicity: • Should not be used as a single therapy • Should not be used in pregnancy • May produce iodism causing acniform rash, swelling of salivary glands, mucous membrane ulceration, metallic taste bleeding disorders and rarely anaphylaxis.
RADIOACTIVE IODINE • 131 I isotope , administered orally • It is rapidly absorbed, concentrated in thyroid gland and stored in follicles. • It has a half life of 5 days • It is easy to administer ,effective , painless and less expensive • It causes destruction of parenchyma ,necrosis and follicular disruption.
Radio active iodine cont’d • Therapeutic effect is due to emission of β-rays. • Patients with age above 40 years only can be treated with this • It crosses placenta and excreted in breast milk • It may cause genetic damage and leukemia and neoplasia ,it may be carcinogenic
IODINATED CONTRAST MEDIA • Ipodate , iopanoic acid administered orally • Diattrizoate administered intravenously • These drugs rapidly inhibit the conversion of T4 to T3. • They are relatively non toxic • Useful adjunctive therapy in thyroid storm • Valuable alternative when thioamides or iodidescontraindicated.
ADRENOCEPTOR BLOCKING AGENTS: • Many symptoms of thyrotoxicosis mimic , especially those which are associated with sympathetic stimulation. • Beta blocking drugs without intrinsic sympathomimic activity are the agents of choice in these conditions e.g. Propranolol. • In conditions where Beta blockers cannot be used then Diltiazem is used.