Download
1 / 1
10 likes | 152 Views
EXERCISE-ASSOCIATED HYPONATREMIA: THE EFFECTS OF CARBOHYDRATE AND HYDRATION STATUS ON IL-6, ADH, AND SODIUM CONCENTRATIONS. Kimberly A. Hubing 1 , Laura R. Quigg 1 , John T. Bassett 1 , Melody D. Phillips 1 , James J. Barbee 2 , and Joel B. Mitchell 1 FACSM, 1

E N D
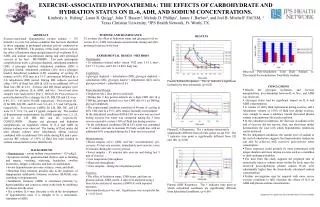
EXERCISE-ASSOCIATED HYPONATREMIA: THE EFFECTS OF CARBOHYDRATE AND HYDRATION STATUS ON IL-6, ADH, AND SODIUM CONCENTRATIONS. Kimberly A. Hubing1, Laura R. Quigg1, John T. Bassett1, Melody D. Phillips1, James J. Barbee2, and Joel B. Mitchell1 FACSM, 1 Texas Christian University, 2JPS Health Network, Ft. Worth, TX. TCU Kinesiology Ex. Phys. Lab PURPOSE AND SIGNIFICANCE To evaluate the effect of hydration status and glycogen level on venous IL-6, ADH, and sodium concentrations during and after prolonged exercise in the heat. ABSTRACT Exercise-associated hyponatremia (serum sodium < 135 mmol/L) is a rare, but serious condition that has been identified in those engaging in prolonged, physical activity conducted in the heat. PURPOSE: The purpose of this study was to evaluate the effect of hydration status and glycogen level on plasma IL-6, ADH, and sodium concentrations during and after prolonged exercise in the heat. METHODS: Ten male participants completed four trials: a glycogen depleted, euhydrated condition (DE); a glycogen depleted, dehydrated condition (DD); a glycogen loaded, euhydrated condition (LE); and a glycogen loaded, dehydrated condition (LD) consisting of cycling 90 minutes at 60% VO2 max in a 35˚C environment followed by a 3-h rehydration (RH) period. During RH, subjects received either 150% of fluid lost (DD & LD) or an additional 50% of fluid lost (DE & LE). Exercise and RH blood samples were analyzed for glucose, IL-6, ADH, and Na+. Sweat and urine samples were analyzed for [Na+]. RESULTS: Post-exercise to post-rehydration [Na+] changes for LD, DD, DE and LE were -6.85, -6.7, -1.45 and 0.10 mM, respectively. Post-exercise [IL-6] for DD, LD, DE, and LE were 5.4, 4.0, 3.7, and 3.49 pg/mL, respectively. Post-exercise [ADH] for LD, DD, DE, and LE were 21.5, 12.8, 7.6, and 1.9 pg/mL, respectively. The number of hyponatremic measurements for all RH samples was 5, 5, 20, and 10 for LD, DD, DE, and LE, respectively. CONCLUSION: Despite our glycogen and hydration manipulations, no regulatory effects of IL-6 and ADH on plasma sodium were observed. The timing of fluid intake did alter plasma sodium since euhydration during exercise combined with an additional 50% intake during RH, and a post-exercise RH volume of 150% of fluid lost both resulted in sodium concentrations below initial levels. • Observed Post-rehydration Total Body Sodium vs. Theoretical Post-rehydration Total Body Sodium. • CONCLUSIONS • Despite the glycogen, hydration, and exercise manipulations, no relationship between IL-6, Na+, and ADH was observed. • Glycogen status had no significant impact on IL-6 and ADH concentrations. • A volume of 100% fluid replacement during exercise, and a rehydration volume of 150% of fluid lost during exercise, were enough to cause a tendency toward decreased plasma sodium concentrations after each condition. • In the euhydrated conditions, the decrease in sodium at the end of exercise did not recover; thus, our short-term model demonstrates the ease with which hyponatremic tendencies can be achieved. • In the dehydrated conditions, the similar level of sodium at the end of rehydration suggests that hyponatremic tendencies can also be achieved with excessive post-exercise water consumption. • These responses could possibly be more pronounced with longer duration and more intense exercise such as a marathon or ultra-endurance triathlon. • The data from this study supports the proposed idea of osmotically inactive sodium stores within the body since the observed post-rehydration plasma sodium levels were substantially higher than the theoretically calculated sodium concentrations. • Further investigation may be required with more severe exercise conditions to fully elucidate the effects of IL-6 on ADH and plasma sodium concentrations. Supported by a grant from the Gatorade Sports Science Institute RESULTS Plasma Sodium Responses. The @ indicates a significant hydration by time interaction. (p=0.02) Plasma IL-6 Responses. The indicates time point is significantly different from all time points except 180. The † indicates time point is significantly different from 120 and 180. (p=0.00) Plasma ADH Responses. The * indicates time point at which euhydrated conditions are significantly different from dehydrated conditions. (p=0.00) • EXPERIMENTAL DESIGN / METHODS • Participants: • 10 endurance-trained males (mean VO2 max 3.61 L·min-1, 24.2 7.6 years, and 9.28 4.88% body fat). • Conditions: • glycogen depleted + dehydration (DD); glycogen depleted + euhydration (DE); glycogen loaded + dehydration (LD); and a glycogen loaded + euhydration (LE). • Experimental Design: • Depletion ride 2 days prior to each trial. • During this 2 day period subjects ate a high CHO diet (8 g CHO/kg; glycogen loaded) or a low CHO diet (0.5 g CHO/kg; glycogen depleted). • The experimental condition consisted of 90 min of cycling at 60% VO2 max in a 35˚C, 40% relative humidity environment. • In the dehydrated conditions (DD & LD) no water was received during exercise but water was consumed during the 3 hour recovery period to restore 150% of fluid loss during exercise. • In the euhydrated conditions (DE & LE) water was consumed at 15 minute intervals to maintain 0% body weight loss with an additional 50% consumed during the 3 hour recovery period. • Measurements: • Blood samples (IL-6, ADH, and Na+ concentrations): pre-exercise, 45 min into exercise, immediately post exercise, every 30 minutes during the recovery period. • Sweat samples – 45 minutes into exercise and during last 5 min of exercise • Core temperature (throughout) • Heart rate (throughout) • Urine samples – during the rehydration period • Statistics: • The effect of hydration status, CHO status, and time on plasma sodium, ADH, and IL-6 data were analyzed using a three factor analysis of variance (ANOVA) with repeated measures. • Newman-Keuls post hoc test. Significance was accepted at the p < 0.05 level. • BACKGROUND • Hyponatremia = serum sodium concentrations < 135 mEq/L. • Symptoms include: gastrointestinal distress such as bloating and nausea, vomiting, wheezing, headaches, swollen extremities, fatigue, confusion, and lack of coordination. • Severe hyponatremia can cause seizures, coma, and death. • Abnormal fluid retention, possibly due to the syndrome of inappropriate antidiuretic hormone secretion (SIADH), may contribute to hyponatremia • Antidiuretic hormone (ADH) is stimulated primarily by hyperosmolality and conserves water in the body by inhibiting its release into the urine. • The cytokine IL-6 may also play a role in the development of hyponatremia since it is thought to be a nonosmotic stimulator of ADH.


















