Download
1 / 37
400 likes | 739 Views
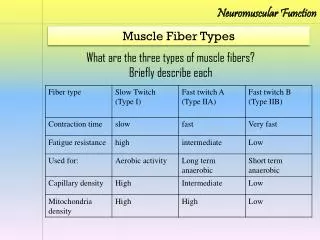
Neuromuscular Emergencies. Hanni Bouma. Objectives. Discuss the approach to neuromuscular respiratory failure Signs & Symptoms Differential diagnosis When to intubate Brief overview of GBS & MG. Case 1.

E N D
Neuromuscular Emergencies Hanni Bouma
Objectives • Discuss the approach to neuromuscular respiratory failure • Signs & Symptoms • Differential diagnosis • When to intubate • Brief overview of GBS & MG
Case 1 • 26 yo previously healthy F p/w tingling in feet since 1 week ago. Two days later noticed difficulty climbing stairs, followed by weakness of her arms. She is areflexic. • What percentage of patients with her disease develop resp failure?
Case 1 • A) 5% • B) 10 to 20% • C) 25 to 50% • D) 70 to 85%
Case 2 • 73 yo M adm w/ 3-month history of progressive proximal weakness • 1 day after muscle biopsy, noticed on rounds to be breathless • What are we likely to see if this patient is in resp failure?
Case 2 • A) Significant accessory muscle use • B) Pt complaining that “I can’t breathe!” • C) Shallow breaths; weak cough; neck flexor weakness • D) Able to count to 40 in a single breath
Case 3 • 63 yo M with limb-onset ALS since 2007 p/w choking sensation, difficulty “getting air in” • Not on home BiPAP • No prior aspiration pneumonias; no fever, no leukocytosis
Case 3 • Which of the following are you LEAST likely to find in this patient? • A) FVC 1.1 L, MIP -20, MEP 30 • B) MEP 40, MIP unable to complete • C) pH 7.35, pCO2 60, bicarb 36 • D) FVC 4 L, MIP -90, MEP 100
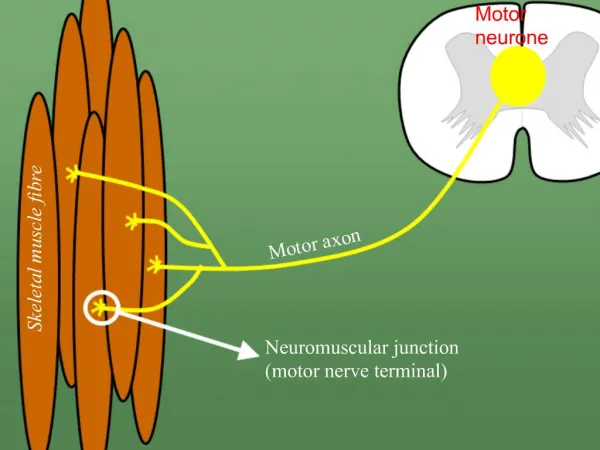
What can cause generalized weakness leading to resp failure? • Spinal cord lesion • Cervical cord compression, transverse myelitis • Motor neuron lesion • ALS • Peripheral nerve lesion • GBS, CIDP, critical illness polyneuropathy, Lyme disease, tick paralysis, toxic • NMJ disorder • MG, LEMS, botulism, organophosphate poisoning • Muscle lesion • Polymyositis, dermatomyositis, critical illness myopathy, hyperthyroidism, congenital myopathy (muscular dystrophy), mitochrondrial myopathy
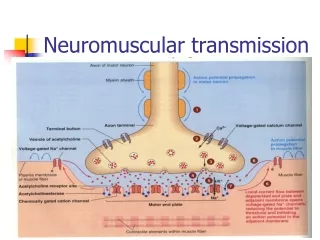
Mechanisms of NM resp failure 1) Upper airway obstruction: • Facial, oropharyngeal, laryngeal weakness mechanical obstruction in supine position • impaired swallowing/secretion clearance aspiration 2) Inspiratory muscle weakness atelectasis V/Q mismatch hypoxia 3) Expiratory muscle weakness weak cough/poor secretion clearance aspiration & pneumonia 4) Acute complications PE, pneumonia, etc.
History • Time course? • progressive weakness over hours to days GBS • fluctuating weakness (on an hourly basis) present for weeks/months MG • Distribution of weakness? • Proximal > distal (MG & GBS) • Ascending in GBS • Initally EOM/oropharyngeal muscle weakness, then generalizes in botulism • Sensory Sx.? • Distal paresthesias common in GBS • No sensory inv’t in MG
History • Pain? • Low backache frequently in GBS; neck pain: C-spine lesion? • Antecedent illness? • 60% of GBS triggered by viral URT illness or C.jejuni gastro • 40% of myasthenic crises triggered by infection • Medications • Exposure to fertilizers & pesticides? • Organophosphate poisoning • Recent diet • Botulism from home-canned goods
Exam: Signs of resp failure • Tachycardia • Rapid, shallow breathing • Stridor • Weak cough, nasal voice, pooling of saliva (signs of bulbar dysfunction) • Orthopnea (abnormal if VC drops >10% supine) • Staccato speech = the need to pause between words • Abdominal paradox = diaphragm weakness • weakness of neck & trapezius muscles (parallels diaphragm weakness) • Single-breath count: ask them to inhale fully & count from 1 to 50. If <25, sign of severe impairment of VC Mehta, S. “Neuromuscular disease causing acute respiratory failure.” Respiratory Care, 2006. 51 (9): 1016-1023.
Focused exam • HEENT: • look for pooled secretions • Swallow test • Dysphonia (nasal voice from palatal paralysis) • Dysarthria • Lungs • Diaphragm: observe/palpate for normal, outward abdominal movement with inspiration • Cough strength • Count test (1 to 50)
Neuro exam • CNs • Pupils: • Reactivity may be lost in botulism or Miller-Fisher variant of GBS • EOM: • weakness + ptosis characteristic of MG, but also seen in MF, botulism, etc. • Face, palate, tongue, & neck strength • Motor exam: • Fasciculations? (ALS, organophosphate poisoning); tone; power (distribution of weakness? Fatigable weakness?) • Sensory: • Distal sensory loss in GBS • Sensory level at C-spine level w/ quadriparesis = C-spine lesion • Coordination: • Ataxia in MF variant of GBS • Reflexes: • Areflexia in GBS; usually preserved reflexes in MG
Investigations • Bedside PFTs:“20/30/40 rule” • Vital capacity (max exhaled volume after full inspiration). Normal = 60 ml/kg (4 L in 70 kg person). VC < 20 ml/kg (or 1 L) means intubation • Max inspiratory pressure. Index of ability to avoid atelectasis. Normal = <-50 cm H2O. MIP >-30 means intubation • Max expiratory pressure. Index of ability to cough/clear secretions. Normal >60 cm H2O. MEP <40 means intubation • PFTs may be low if inadequate mouth closure from facial palsy, and may fluctuate in MG
Investigations • ABG: • Hypercarbia (PCO2 > 45 mmHg) = hypoventilation * PCO2 often normal or low until late in NM resp failure • Hypoxia (PO2 < 75 mmHg) = V/Q mismatch usually atelectasis or pneumonia in this setting
Investigations • Basic labs (CBC, SMA-10, LFTs, CK) • CXR • EKG (electrolyte D/O; GBS ass’d w/ dysautonomia arrhythmias)
General care • Electrolytes: low potassium, high magnesium & low phosphate exacerbate muscle weakness • Serial PFTs (MIP/MEP/FVC) bid to qid • Chest physio, suctioning& incentive spirometry • DVT prophylaxis • HOB elevation • NPO if bulbar weakness; NG or Dobhoff feeding • Bowel/bladder: paralysis predisposes to constipation; GBS pts may have urinary retention
Determine: • If resp failure is imminent • If ICUshould be involved • What is the localization?
Predictors of need for MV • 20/30/40 rule • or a reduction in VC, MIP, MEP by >30% • PO2 <70 mmHg on RA or PCO2 >50 mmHg w/ acidosis • Dysarthria, dysphagia, impaired gag reflex • In GBS: • Time from onset to admission < 7 days • Inability to cough • Inability to stand • Inability to lift elbows or head • LFT increases • Presence of autonomic dysfxn Sharshar T, Chevret S, Bourdain F, Raphael JC. Early predictors of mechanical ventilation in Guillain-Barre´ syndrome. Crit Care Med 2003;31(1):278–283.
Intubation: things to think about • Code status? • Identify imminent resp failure early to avoid emergency intubation • Minimizes atelectasis/pneumonia • Minimizes complications of intubation specific to GBS & MG: • Dysautonomia: can cause severe bradycardia, BP shifts, profound hypotension w/ sedatives • Denervated muscle: can cause fatal hyperkalemia with use of succinylcholine • Avoid depolarizing NM blockers • Small doses of benzos
NPPV? • Few studies on its use in GBS & MG • Inappropriate if upper airway function severely impaired or hypercapnic resp failure
GBS • Most common cause of acute or subacute gen’d paralysis • Monophasic AIDP: autoimmune attack against surface antigens on peripheral nerves • Develops 5 days to 3 weeks after resp/GI infection in 60% • Campylobacter jejuni (26%) • Viral URTI, influenza • EBV, CMV, VZV, HIV, hep A & B, coxsackie • Other precipitants: immunization, pregnancy, surgery, Hodgkin’s disease
Presentation • Sensory: • distal paresthesias/numbness (earliest Sx.) • Reduced vibration/proprioception • Motor: • Symmetric; evolves over days to 1-2 wks • Ascending: LE before UE; proximal> distal • May progress to involve trunk, intercostals, neck, bulbar, B/L FNs • Median duration from onset to max weakness 12 days • Reflexes: reduced, then absent • Autonomic instability: • Sinus tachy/brady, arrhythmias, labile BP (esp hypertension), urinary retention, anhydrosis • Other: low backache very common, myalgias
Investigations • EMG: • Reduced conduction velocities • Loss of F waves • Conduction block in motor nerves • Reduced motor amplitudes: 2° axonal damage worse Px. • CSF: • High protein (may be normal in first 2 days) • No cells or few lymphs • 10% have 10-50 lymphs
Management • Admit for observation (potential for deterioration) • Determine if resp failure imminent • Dysautonomia: most frequently sustained HTN & tachycardia • Esp in older pts w/ CAD, consider Labetolol • Hypotension in 10% fluids, pressors • PLEX (4-6 Rx. q1-2d) & IVIG (0.4g/kg/d x 5 d): • Equally effective • PLEX useful in first 2 weeks; benefit less clear after that • Steroids no proven benefit
Course • Progression over 1-4 weeks • Plateau: 2-4 months • Recovery: few wks to months • Mortality 3-5% • Poor prognosis: • Resp failure requiring intubation • Advanced age • Very low distal motor amplitudes (axonal damage) • Rapidly progressive weakness over 1 week
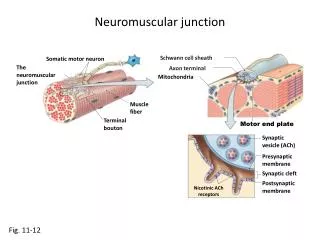
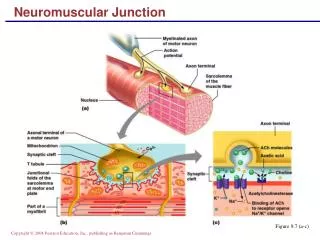
MG • Ab-mediated attack on nicotinic Ach rec defective transmission across NMJ • Bimodal: F 20-30 yo; M 50-60 yo • 2 autoimmune forms • Ach receptor Ab+: 80% with generalized MG & 50% with ocular MG • Anti-MuSK Ab+: 50% of patients who are Ach rec Ab negative; typically female with prominent bulbar weakness
Presentation • Motor: • Fluctuating, fatigable weakness involving eyes (90%), face/neck/oropharynx (80%), limbs (60%) • Limbs rarely affected in isolation • Rest restores strength (at least partially) • Usually insidious onset • Sensory: normal • Reflexes: preserved • Thymic abnormalities: • Malignant thymoma in 10-15% (more severe disease) • Thymic hyperplasia in 50-70%
Myasthenic Crisis • Defined by resp failure requiring ventilatory assistance • Occurs in 20-30%; mortality 5% • Common precipitants: • Infection in 40% (esp respiratory) • Pregnancy • Medications • Aspiration • Surgery • Emotional upset, hot environment
Drugs that exacerbate MG • Antibiotics: • Aminoglycosides (genta, tobra) • Fluroquinolones (cipro) • Macrolides (erythromycin, azithro, tetracycline, doxycycline) • Cardiac: • All beta-blockers • Calcium channel blockers • Class I anti-arrhythmics (quinidine, procainamide) • Anticonvulsants: • Phenytoin, CBZ • Antipsychotics, lithium • Thyroid hormones • Magnesium toxicity • Iodinated contrast agents • Muscle relaxants • Baclofen • Long-acting benzos • **Too much anticholinesterase
Investigations • Ach receptor Abs • Anti-MuSK Abs • EMG: • Repetitive nerve stimulation: >10% decrement in amplitude betw 1st & 5th CMAP • Sens/spec 90% when weak, proximal muscles stimulated; <50% sens in pts w/o limb weakness • Single-fiber: “jitter” (variation in time interval betw firing of muscle fibers in same motor unit) • Sens >95% for MG but not specific • Edrophonium (Tensilon) test: • Not recommended in suspected crisis
Management • Determine if resp failure imminent • Stop exacerbating meds • Treat infection • Symptomatic therapy (mild-moderate weakness): • Cholinesterase inhibitors (Mestinon) • Short-term disease suppression: • To hasten clinical improvement in hospitalized pts w/ crisis or impending crisis; pre-operatively; chronic refractory disease • PLEX: improvement w/i days, but lasts only 2-4 wks • IVIG: benefit may last up to 30 days • Comparable benefits • Long-term immunosuppression: • When weakness is inadequately controlled by Mestinon • Prednisone • Azathioprine (if steroid failure or excessive SE)
Key points • 20/30/40 rule • Identify pts at risk for resp failure EARLY to avoid emergency intubation • Don’t wait for pts to complain of SOB before doing bedside PFTs