Download
1 / 34
340 likes | 535 Views
Suicide and Alaska- some special topics. Richard Ries MD rries@u.washington.edu Harborview Medical Center and the University of Washington Seattle, Washington. Ries Conflict of Interest Statement. Dr Ries is on Speaker’s bureaus for Janssen, and Alkermes Dr Ries has Grant funding from:

E N D
Suicide and Alaska-some special topics Richard Ries MD rries@u.washington.edu Harborview Medical Center and the University of Washington Seattle, Washington RRies Addiction and Suicide
Ries Conflict of Interest Statement • Dr Ries is on Speaker’s bureaus for • Janssen, and Alkermes • Dr Ries has Grant funding from: • NIH- NIDA • Contingency Management Meth in Mentally Ill • Preventing Addiction Related Suicide • Brief Interventions of Drug Abuse in Prim Care • CSAT • National Co-occurring Center of Excellence • DOD- Suicide Prevention grant
Some Facts about Suicide: • 30,000 die by suicide in USA each year • More die by suicide than homicide (1.7 times more) • Third leading cause of death in those 15-24 ….more than cancer, AIDS, heart, and lung disease combined • Males die 4x more often, but females make more attempts • 60% die by firearm CDC web site
Facts about Suicide: • 500,000 ER visits for attempts in 1997 • Four times as many US citizens died by suicide during the Viet Nam War period than died as soldiers. • Rates increase with age ( as do other causes of death) • Often Drug/Alcohol related CDC web site
Risk and Lethality • Risk of Attempt • Previous attempt • Family History of Suicide • Psychiatric disorder • Alcohol/Drug disorder • Alcohol/Drug Intoxication • Loss • Hopelessness/end of rope • Risk of Lethality • Male 4/1 over females • Guns 70% • Access • Older >70 • Alone/Loss of support • Alcohol • Serious illness • Medical • Psychiatric
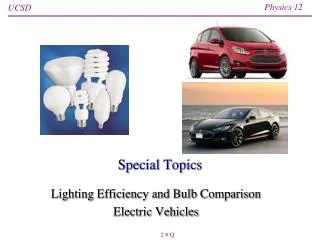
2009, United States Suicide Injury Deaths and Rates per 100,000 All Races, Both Sexes, All Ages ICD-10 Codes: X60-X84, Y87.0,*U03
HOW U.S. SOLDIERS DIE Suicide accounted for an average of nearly 1 in 5 deaths among regular and reserve U.S. military personnel between October 1998 and September 2003. Source: U.S. Armed Forces Medical Examiner, 2004
J Sch Health. 2004 May;74(5):177-82. Attempted Suicide and associated health risk behaviors among Native American high school students. Shaughnessy L, Doshi SR, The study included students in BIA-funded high schools with 10 or more students enrolled in grades 9-12. Overall, 16% of BIA high school students attempted suicide one or more times in the 12 months preceding the survey. Risk Factors: > unintentional injury and violence behaviors, > sexual risk behaviors, > tobacco use, and > alcohol and other drug use.
What about Addiction and Suicide ? • Lifetime Suicide risk for Schizophrenic, Affective and Addiction Disorders: • Method: review of 83 mortality studies: • Schizophrenia…………4% • Affective Disorders……6% • Addiction Disorders…...7% Inskip HM: Br J Psych 1998
Is Suicide also Addictions Territory? Alcohol strongest predictor of completed suicide over 5-10 years after attempt, OR= 5.18…vs. demog or psych disorders ( Beck J Stud Alc 1989) 40-60% of completed suicides across USA/Europe are alcohol/drug affected (Editorial: Dying for a Drink: Brit Med J. 2001) Higher suicide rates (+8%) in 18 vs. 21yo legal drinking age states for those ages (Birckmayer J: Am J Pub Health 1999)
Lifetime Suicide Thoughts/Attempts N=60,952
What do we know about Suicide Attempts in Prospective Age-Matched Alcoholic Populations • 4.5% of alcoholics attempted suicide within 5 years of DX • ( age 40.. n=1,237) • 0.8% in non-alcoholic matched comparison group • ( age 42..n=2,000)… • p< .001……….. 700 % increased risk of Suicide Attempts Preuss/Schuckit Am J Psych 03
What Predicted Suicide Attempts in Alcoholics (n=1,237) over 5 years? • Rate = 4.5% attempted suicide • Prior attempts • Earlier onset and more severe dependence. Other drug dependence • Separated or divorced • More likely to have had treatment ( more severe) • More Panic • More Substance Induced Psych Disorder Preuss/Schuckit et al Am J Psych03
1: Drug Alcohol Rev. 2005 May;24(3):203-8. Alcohol and suicide at the population level--the Canadian experience. Ramstedt M. Studies suggest that the population level link between alcohol and suicide differs across countries and between men and women. The aim of this paper was to estimate the relationship between alcohol consumption and suicide in Canada and to put the results in a comparative perspective. The total suicide rate in Canada increased significantly by around 4% as alcohol consumption increased by one litre per capita, suggesting that approximately 25 - 30% of Canadian suicides were related to alcohol.
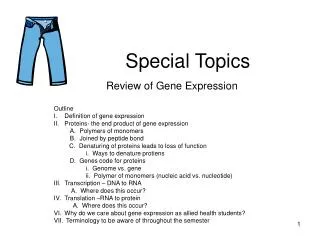
Standardized suicide mortality rates in men and women with mean annual alcohol consumption in litersper capita. Russia1965-99. Suicide in Women Suicide in Men Alcohol Consumption Men Women
Mean annual consumption with BAC-positives and BAC-negatives for 8 Russian Regions 1981-1990. Alcohol consumption Suicide Rates per 100,000 BAC Positive Suicides BAC Negative Suicides Alcohol Consumption
Substance Induced Depression: Severity/Dangerousness Henriksson, et al (1993)- 43% of completed suicides had alcohol dependence. 48% of these were also depressed. 42% had a personality disorder. Elliot, et al (1996)- patients with medically severe suicide attempts had a statistically higher prevalence or substance-induced mood disorder. Pages K et al (1997)- Higher degrees of Sub Dep related to higher severity suicide ratings
METH ADDICTS: LIFETIME SUICIDE ATTEMPTS, BEHAVIOR PROBLEMS, AND FELONY CHARGES, BY GENDER Zweben, et al., 2004
Suicide rates in clinical trials of SSRIs, other antidepressants, and placebo: analysis of FDA reports.Khan A, Khan S, Kolts R, Brown WA. • RESULTS: Of 48,277 depressed patients participating in the trials, 77 committed suicide. Based on patient exposure years, similar suicide rates were seen among those randomly assigned to an SSRI (0.59%, 95% confidence interval [CI]=0.31%-0.87%), a standard comparison antidepressant (0.76%, 95% CI=0.49%-1.03%), or placebo (0.45%, 95% CI=0.01%-0.89%). • CONCLUSIONS: These findings fail to support either an overall difference in suicide risk between antidepressant- and placebo-treated depressed subjectsin controlled trials or a difference between SSRIs and either other types of antidepressants or placebo.
Can addiction treatment affect suicidality? Cohort suicide attempts Adults Year Prior Year After > 25 yo (n=3524) 23%...........................4% 18-24 yo (N=651) 28%...........................4% Adoles (n=236) 23%...........................7% Karageorge: National Treatment Improvement Evaluation study 2001
Alcohol Consumption, Alcoholics Anonymous membership, and Suicide MortalityRates, Ontario, 1968-1991.Mann RE, Zalcman RF, Smart RG, Rush BR, Suurvali H.Method: We studied the impact of alcohol consumption levels, AA membershiprates, and unemployment rates on suicide mortality rates in Ontario from 1968 to1991. Results: Total alcohol consumption was significantly and positively related to total and female suicide mortality rates. AA membership rates were negatively related to total and female suicide rates. (J. Stud. Alcohol 67: 445-453, 2006).
Opioid Related Death Hulse, English, Mline, & Holman, 1999; Seymour et al. 2000, CDC 2010, 2012 • Opiates and Opioids have the highest death rates of any psychoactive illicit-substances • Accidental deaths from Prescription Opioids now Outnumber Traffic deaths in many states • The 2010 CDC report, Unintentional drug poisoning in the United states, sites heroin and prescription painkillers as the two leading causes of overdose death in the US
Overdose Planned LethalityFully accidental Just blot out worries Who cares if I wake Lethal Plan
Opioid Deaths • Mortality rate of opioid users 14 times that of general population • 46% to 70% of opioid users experience one or more non-lethal overdoses during their lifetime • Opiate users who were recently released from prison were at even higher risk of overdose, and this risk may also exist post “Detox”
Suicide and Opiates • 1 in 5 (20%) of suicide victims have opiates in their bodies at time of death, including heroin, and prescription painkillers • Opioid dependent adults are 14 times more likely that their non-drug using counterparts to die by suicide Between 33% and 50% of drug users have a history of suicide attempts • Suicide accounts for an estimated 3% to 35% of deaths among heroin users • Spectrum of Volition— • Accidental -- Risky -- Passive SI -- Planned Suicide Harris and Barraclough, 1997; Darke and Ross, 2002, Ries SPOT unpub
Male gender Suicide Accidental Overdose Previous attempt Depression Previous overdose Personality Disorder: CCD ASPD Social isolation Homelessness Poly-substance abuse Genetic predisposition Hx. of childhood sexual trauma Risk Factors for Suicide in Opiate Abusers Parallel Risk Factors for Accidental Overdose(Darke and Ross, 2002)
Evidence Supported Overdose Prevention Programs Prevention of Fatal overdose Gunne and Gronbladhm, 1981; Bammer, 2000; McGregor, Ali Christie, Darke, 2001 Methadone: opiate replacement therapies reduce opiate overdose risk by 75% Naloxone: ER administered Naloxone, peer administered Naloxone (I.M., I.V., S.Q., intranasil). Medically supervised injection facilities: report 0 fatal overdose deaths. Educational programs: presented at needle exchange programs Protocols: limiting police intervention in during overdose emergencies
Preventing Addiction Related Suicie (PARS) NIDA R21Ries, Voss, Comtois, Addictions staff and directors Designed to be a single 3 hour IOP session integrated into typical outpt Addictions Treatment programs—for all patients in treatment To enhance positive changes in Attitudes, Knowledge, and Adaptive Skills for suicidal issues in both patients and those around them, workbook based, Needing only a single 3 hour staff training session—using same guide they then use to perform and guide group. Designed iterively with REAL WORLD addictions staff, administrators, and patients for feasabiity RETRAINS STAFF EACH TIME USED IN IOP, OR OTHER FORMAT
Suicide Resources: American Association of Suicidology: www.suicidology.org American Foundation for Suicide Prevention: www.afsp.org National Strategy for Suicide Prevention: www.mentalhealth.org/suicideprevention/ National Suicide Prevention Strategy www.sg.gov/library/calltoaction/ CDC
Suicide Resources: Suicide Prevention Advocacy Network (SPAN) www.spanusa.org QPR institute: www.qprinstitute.com Substance Abuse and Mental Health Services Administration: www.samhsa.gov Tip 50- Addiction and Suicide www.CSAT.gov
Now lets talk about some of YOUR issues Suicide Assessment Suicide prevention Suicide Treatment